Vous aimerez peut-être aussi
- Turf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandTurf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentD'EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiPas encore d'évaluation
- Fai 2007 0529Document7 pagesFai 2007 0529milenabogojevskaPas encore d'évaluation
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoPas encore d'évaluation
- Coste Et Al. - 1968 - Rheumatoid ForefootDocument2 pagesCoste Et Al. - 1968 - Rheumatoid ForefootYuki SATAKEPas encore d'évaluation
- Osteotomies For Bunionette Deformity: Lowell Weil JR,, Lowell Scott Weil SRDocument24 pagesOsteotomies For Bunionette Deformity: Lowell Weil JR,, Lowell Scott Weil SRMiguel Angel Palacios FloresPas encore d'évaluation
- Comminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewDocument7 pagesComminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewGustavoBecerraPas encore d'évaluation
- Subtrochanteric Femur Fractures: Current Review of ManagementDocument7 pagesSubtrochanteric Femur Fractures: Current Review of ManagementErmiPas encore d'évaluation
- Guía de Práctica Clínica para El Tratamiento de Fractura de RótulaDocument8 pagesGuía de Práctica Clínica para El Tratamiento de Fractura de Rótulabarbara liuva chia policarpoPas encore d'évaluation
- Functional Bracing Fractures PDFDocument10 pagesFunctional Bracing Fractures PDFPPVRM100% (1)
- Davis Modified Lingual Split 1983Document7 pagesDavis Modified Lingual Split 1983ArchanaShenoyPas encore d'évaluation
- Adult FlatfootDocument7 pagesAdult FlatfootAbraham SaldañaPas encore d'évaluation
- Hallux AlgorithmDocument15 pagesHallux AlgorithmMohamed SalehPas encore d'évaluation
- Metatarsalgia Besse2017Document11 pagesMetatarsalgia Besse2017suad5stambuliePas encore d'évaluation
- Anterograde Percutaneous Treatment of Lesser Metatarsal Fractures Technical Description and Clinical ResultsDocument5 pagesAnterograde Percutaneous Treatment of Lesser Metatarsal Fractures Technical Description and Clinical ResultsRoyman MejiaPas encore d'évaluation
- Stability in Ankle Fractures Diagnosis and TreatmeDocument10 pagesStability in Ankle Fractures Diagnosis and TreatmeAryo WibisonoPas encore d'évaluation
- Maxillary Orthognathic Surgery: Richard E. Bauer III,, Mark W. OchsDocument15 pagesMaxillary Orthognathic Surgery: Richard E. Bauer III,, Mark W. OchsMariaPas encore d'évaluation
- 2021 - Chronic Isolated Radial Head DislocationDocument9 pages2021 - Chronic Isolated Radial Head Dislocationjuan pablo aguirrePas encore d'évaluation
- The Failed Hallux ValgusDocument127 pagesThe Failed Hallux ValgusFlorin MacariePas encore d'évaluation
- General Considerations: Metatarsals - 1st, Head, Intraarticular T-TypeDocument9 pagesGeneral Considerations: Metatarsals - 1st, Head, Intraarticular T-Typenovalin23Pas encore d'évaluation
- Alingment in TKRDocument3 pagesAlingment in TKRdeepak100% (1)
- Soft Tissue Balance KneeDocument10 pagesSoft Tissue Balance KneeNitin BansalPas encore d'évaluation
- Percutaneous Osteotomies in Pediatric Deformity Correction: Nickolas Nahm,, Louise Reid Boyce NicholsDocument16 pagesPercutaneous Osteotomies in Pediatric Deformity Correction: Nickolas Nahm,, Louise Reid Boyce NicholsAnonymous kdBDppigEPas encore d'évaluation
- Lesser Metatarsal Osteotomy Complications: Lowell S. Weil and Erin E. KleinDocument9 pagesLesser Metatarsal Osteotomy Complications: Lowell S. Weil and Erin E. KleinAntonio FloresPas encore d'évaluation
- Fractura e FalangsDocument16 pagesFractura e FalangsJulio Cesar Guillen MoralesPas encore d'évaluation
- Ankle FracturesDocument9 pagesAnkle FracturesUmar Dion SiraidPas encore d'évaluation
- Strategies To Improve Outcomes From Operative Childhood Management of DDHDocument9 pagesStrategies To Improve Outcomes From Operative Childhood Management of DDHVALENTINA LOPEZ MARINPas encore d'évaluation
- Ehlinger (2010)Document6 pagesEhlinger (2010)TommysPas encore d'évaluation
- Modul Hip Disarticulation ProstheticsDocument67 pagesModul Hip Disarticulation ProstheticsCapt KidsPas encore d'évaluation
- Currentmanagementof Metacarpalfractures: Rafael Diaz-Garcia,, Jennifer F. WaljeeDocument12 pagesCurrentmanagementof Metacarpalfractures: Rafael Diaz-Garcia,, Jennifer F. WaljeeHarry CenPas encore d'évaluation
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíPas encore d'évaluation
- Ankle FractureDocument4 pagesAnkle FracturerheyasrPas encore d'évaluation
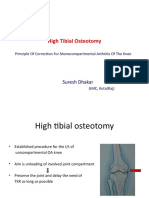
- High Tibial Osteotomy: Suresh DhakarDocument40 pagesHigh Tibial Osteotomy: Suresh DhakarAtul PandeyPas encore d'évaluation
- Jurnal Fraktur TibiaDocument8 pagesJurnal Fraktur TibiaAnggi CalapiPas encore d'évaluation
- Motec Wrist Sales Brochure - P125-28!1!20191204Document20 pagesMotec Wrist Sales Brochure - P125-28!1!20191204ThúyPas encore d'évaluation
- FX Leño Verde SagitalDocument6 pagesFX Leño Verde SagitalYury Angelica SierraPas encore d'évaluation
- Foot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Document15 pagesFoot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Biblioteca Centro Médico De Mar del PlataPas encore d'évaluation
- Revision of Failed Bunion SurgeryDocument19 pagesRevision of Failed Bunion SurgeryCarl LarussonPas encore d'évaluation
- Posterior Malleolus Fractures: AnnotationDocument7 pagesPosterior Malleolus Fractures: AnnotationFrigandraSyahputriPas encore d'évaluation
- Hallux VarusDocument18 pagesHallux VarusSneha SutharPas encore d'évaluation
- Proximal Femoral NewDocument34 pagesProximal Femoral NewHimanshu HemantPas encore d'évaluation
- Comminuted Patella FracturesDocument8 pagesComminuted Patella FracturesKirana lupitaPas encore d'évaluation
- Long Bone Fracture Management - Dr. ImanDocument20 pagesLong Bone Fracture Management - Dr. ImanYuliusPas encore d'évaluation
- Indicações e Marcos Anatômicos para Aplicação de Tração de Membros Inferiores - 2016Document6 pagesIndicações e Marcos Anatômicos para Aplicação de Tração de Membros Inferiores - 2016ericagomes.fisioterapeutaPas encore d'évaluation
- Knee Potential RisksDocument84 pagesKnee Potential RisksAnil Chowadary Anil ChowadaryPas encore d'évaluation
- Yar Boro 2016Document13 pagesYar Boro 2016saimanojkosuriPas encore d'évaluation
- Wagner 2021Document17 pagesWagner 2021Biblioteca Centro Médico De Mar del PlataPas encore d'évaluation
- Foot and Ankle DisordersDocument50 pagesFoot and Ankle DisordersnhfbyqvgwhPas encore d'évaluation
- The Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsDocument8 pagesThe Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsanujPas encore d'évaluation
- Patellar Tendon RuptureDocument13 pagesPatellar Tendon Rupturededyalkarni08Pas encore d'évaluation
- 2 - Operative Treatment of Metacarpal and Phalangeal Shaft Fractures-KozinDocument11 pages2 - Operative Treatment of Metacarpal and Phalangeal Shaft Fractures-KozindouglasPas encore d'évaluation
- Pain Rating ScalesDocument22 pagesPain Rating ScalesJMPas encore d'évaluation
- Presented By: DR Venkatesh V Moderator: DR Harish KDocument81 pagesPresented By: DR Venkatesh V Moderator: DR Harish KPankaj VatsaPas encore d'évaluation
- Amputations Below The Knee: Ernest M. Burgess. M.D. Joseph H. Zettl, C.PDocument12 pagesAmputations Below The Knee: Ernest M. Burgess. M.D. Joseph H. Zettl, C.PLuqmanul HakimPas encore d'évaluation
- Quinto SADocument5 pagesQuinto SAFreddy Churata SuriPas encore d'évaluation
- Biomechanics of The Knee: Tibiofemoral JointDocument7 pagesBiomechanics of The Knee: Tibiofemoral JointManuel Azael Rodríguez CigalaPas encore d'évaluation
- Fixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFDocument4 pagesFixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFThomas BowersPas encore d'évaluation
- Illustration of Implants in Total Knee ReplacementDocument5 pagesIllustration of Implants in Total Knee ReplacementInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- MOC Notes 2011 NewDocument181 pagesMOC Notes 2011 NewMohit GuptaPas encore d'évaluation
- 1994 27 PDFDocument9 pages1994 27 PDFMonika Diaz KristyanindaPas encore d'évaluation
- Barangay Anti-Drug Abuse Council (Badac) Training: Activity DesignDocument3 pagesBarangay Anti-Drug Abuse Council (Badac) Training: Activity DesignMaria Fiona Duran Merquita100% (2)
- Effectivity: SY 2016-2017 Document Code: QR - AAD - 001 Revision No.: 00 Issue No.: 01 Date Issued: March 2015Document7 pagesEffectivity: SY 2016-2017 Document Code: QR - AAD - 001 Revision No.: 00 Issue No.: 01 Date Issued: March 2015Sandre WaldenPas encore d'évaluation
- Trastorno de AdaptacionDocument11 pagesTrastorno de AdaptacionEduardo AguilarPas encore d'évaluation
- Exam Table For Shoulder and ElbowDocument17 pagesExam Table For Shoulder and ElbowLouie OkayPas encore d'évaluation
- Birthday Party - Character SketchesDocument2 pagesBirthday Party - Character SketchesDhivyaPas encore d'évaluation
- Schoolgirl: María de Los Ángeles Lizeth Solís Jiménez Teacher: Kenneth Matter: English VDocument16 pagesSchoolgirl: María de Los Ángeles Lizeth Solís Jiménez Teacher: Kenneth Matter: English VAngeles Solis JimenezPas encore d'évaluation
- SMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Document16 pagesSMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Azie HarunPas encore d'évaluation
- The Book of BulkDocument16 pagesThe Book of BulkpopeyeballinaPas encore d'évaluation
- Contractor Safety Management ProcessDocument14 pagesContractor Safety Management Processsrkam100% (2)
- BTPB RepertoryDocument24 pagesBTPB Repertoryanamika mishra100% (1)
- Evacuation Earthquake PlanDocument9 pagesEvacuation Earthquake PlanShane Giacinth AmarilaPas encore d'évaluation
- K4health-The Mhealth Planning Guide Key Considerations For Integrating Mobile Technology Into Health Programs-2015!04!06Document49 pagesK4health-The Mhealth Planning Guide Key Considerations For Integrating Mobile Technology Into Health Programs-2015!04!06DitaMaryaniPas encore d'évaluation
- 491 Exam 1 KEYDocument10 pages491 Exam 1 KEYLily M Mo100% (1)
- Checklist Auditoria SQF 2010Document21 pagesChecklist Auditoria SQF 2010cramirez48Pas encore d'évaluation
- Taylan Competency NeedsDocument32 pagesTaylan Competency NeedsLovejoice Cha NnelPas encore d'évaluation
- Job Contract Agreement Letter PDFDocument4 pagesJob Contract Agreement Letter PDFQazi Yusuf100% (1)
- RULE 1142. Marine Tank Vessel OperationsDocument8 pagesRULE 1142. Marine Tank Vessel OperationsksalvaradoPas encore d'évaluation
- Gerald Kein - Self Hypnosis HandoutDocument5 pagesGerald Kein - Self Hypnosis HandoutBob Cook100% (1)
- Chapter/Topic Name of Student/s Previous GradeDocument1 pageChapter/Topic Name of Student/s Previous GradeKatrizia FauniPas encore d'évaluation
- Gold Medalist ClubDocument18 pagesGold Medalist ClubSmit patelPas encore d'évaluation
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahPas encore d'évaluation
- CPRDocument45 pagesCPRJames Elwood DoyolaPas encore d'évaluation
- Common Sports InjuryDocument71 pagesCommon Sports InjuryGlen Dizon100% (1)
- SF2 Aquarius Set BDocument2 pagesSF2 Aquarius Set BXyzaPas encore d'évaluation
- Agama Dan Spiritualitas Dalam Konteks Kesehatan Dan KeperawatanDocument28 pagesAgama Dan Spiritualitas Dalam Konteks Kesehatan Dan KeperawatanSELVI AQILAHPas encore d'évaluation
- (1875855X - Asian Biomedicine) Identifications of Hordeolum Pathogens and Its Susceptibility To Antimicrobial Agents in Topical and Oral MedicationsDocument6 pages(1875855X - Asian Biomedicine) Identifications of Hordeolum Pathogens and Its Susceptibility To Antimicrobial Agents in Topical and Oral MedicationsSilvia Dwi AgustinPas encore d'évaluation
- Irradiated Foods 2003 PDFDocument52 pagesIrradiated Foods 2003 PDFDiana BratuPas encore d'évaluation
- Risk Management Plan TemplateDocument10 pagesRisk Management Plan Templateamit singh0% (1)
- Substance Use Disorders Among Youth in The Juvenile Justice SystemDocument14 pagesSubstance Use Disorders Among Youth in The Juvenile Justice SystemJames JerryPas encore d'évaluation
- Holistic WellnessDocument541 pagesHolistic WellnessSeba FounderPas encore d'évaluation