Vous aimerez peut-être aussi
- Surgical Site InfectionsDocument5 pagesSurgical Site Infectionsapi-320469090Pas encore d'évaluation
- AnestheticsDocument32 pagesAnestheticsAnkit JainPas encore d'évaluation
- Activity 1Document2 pagesActivity 1Ace Shernyll Son GallanoPas encore d'évaluation
- General AnesthesiaDocument85 pagesGeneral AnesthesiaShalakha Bhardwaj100% (2)
- Opioid Analgesics: Just in Time Training September 2006Document16 pagesOpioid Analgesics: Just in Time Training September 2006Yel CMPas encore d'évaluation
- Adrenocorticosteroids & Adrenocortical Antagonists: Namwase Hadijja KatabiraDocument77 pagesAdrenocorticosteroids & Adrenocortical Antagonists: Namwase Hadijja KatabiraSamson100% (1)
- DrugsDocument155 pagesDrugsAkankshaPas encore d'évaluation
- Drugs at ORDocument16 pagesDrugs at ORAngelo MangibinPas encore d'évaluation
- Morphine (Astramorph) PCADocument2 pagesMorphine (Astramorph) PCAAdrianne Bazo100% (3)
- DrugcardsDocument70 pagesDrugcards2liter100% (2)
- Local Anesthetics HandoutDocument18 pagesLocal Anesthetics HandoutmirfanulhaqPas encore d'évaluation
- Learner Skill ValidationDocument7 pagesLearner Skill ValidationPaul Zantua33% (3)
- Er-Drug StudyDocument41 pagesEr-Drug Studyrc_lacampuinganyahooPas encore d'évaluation
- Substance Disorder 2020Document59 pagesSubstance Disorder 2020dennyzpsPas encore d'évaluation
- Local AnestheticsDocument93 pagesLocal Anestheticsgeetika100% (1)
- Rug Therapy For Heart Failure: Dr. Santhosh RamakrishnaDocument40 pagesRug Therapy For Heart Failure: Dr. Santhosh RamakrishnaNiteesh Kumar SharmaPas encore d'évaluation
- Local Anesthetics (Pharmacology Lecture)Document4 pagesLocal Anesthetics (Pharmacology Lecture)Jay-r Villanueva100% (1)
- MorphineDocument2 pagesMorphineKatie McPeek100% (2)
- Chemotherapy NDocument28 pagesChemotherapy NFaisal MehboobPas encore d'évaluation
- Pharmacology SlidesDocument114 pagesPharmacology Slidesbrandon15000100% (9)
- Adverse Drug ReactionDocument53 pagesAdverse Drug ReactionShruthi ReddyPas encore d'évaluation
- Respiratory System: Antiasthmatic Drugs Cardiac GlycosidesDocument4 pagesRespiratory System: Antiasthmatic Drugs Cardiac GlycosidesNurse HoomanPas encore d'évaluation
- Oxybutynin ChlorideDocument3 pagesOxybutynin Chlorideapi-3797941Pas encore d'évaluation
- Peenchimento Com Acido Hialuronico em Pacientes AsiaticosDocument17 pagesPeenchimento Com Acido Hialuronico em Pacientes AsiaticosDr.Richard F.KühnePas encore d'évaluation
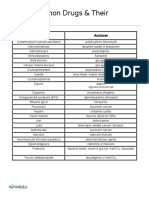
- Drugs and AntidotesDocument1 pageDrugs and AntidoteskiranbhandarkarPas encore d'évaluation
- Pharma Review NotesDocument9 pagesPharma Review NotesYves100% (1)
- Surgical Instrument - Illustration and UsesDocument8 pagesSurgical Instrument - Illustration and UsesJoy Compañero MalabananPas encore d'évaluation
- Inhaled AnesthesiaDocument25 pagesInhaled AnesthesiaazanchePas encore d'évaluation
- Principles of Opioid Management: Symptom GuidelinesDocument45 pagesPrinciples of Opioid Management: Symptom GuidelinesTheresia Avila KurniaPas encore d'évaluation
- AntihistaminesDocument66 pagesAntihistaminesAfif Bastian100% (1)
- Emergency DrugsDocument9 pagesEmergency DrugsaldwinngPas encore d'évaluation
- Ketorolac PI PDFDocument2 pagesKetorolac PI PDFintan kusumaningtyasPas encore d'évaluation
- Antibiotics: Means Against LifeDocument13 pagesAntibiotics: Means Against Lifeshankul kumar100% (1)
- 1.2 Immunity Response TransDocument10 pages1.2 Immunity Response TransJoshua SaanPas encore d'évaluation
- Antibiotic Summary - DraftDocument10 pagesAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Er Drugs StudyDocument80 pagesEr Drugs StudyJobelle AcenaPas encore d'évaluation
- Drug BookDocument30 pagesDrug BookLindy JanePas encore d'évaluation
- Celiac DiseaseDocument37 pagesCeliac DiseaseTaj lamajed100% (1)
- CHAPTER SUMMARY-opiod AnalgesicDocument9 pagesCHAPTER SUMMARY-opiod AnalgesicNuttiya WerawattanachaiPas encore d'évaluation
- Sample Case ScenarioDocument10 pagesSample Case ScenarioKarilee Salcedo AyunayunPas encore d'évaluation
- Desipramine Drug Information - UpToDateDocument32 pagesDesipramine Drug Information - UpToDateWilliam OmarPas encore d'évaluation
- NTP MoP2004Document131 pagesNTP MoP2004meldestacamentojrPas encore d'évaluation
- RD ChecklistDocument14 pagesRD Checklistwerismy daddyPas encore d'évaluation
- Adrenocorticosteroids and Adrenocortical AntagonistsDocument53 pagesAdrenocorticosteroids and Adrenocortical AntagonistsKetan PatelPas encore d'évaluation
- HomatropinDocument11 pagesHomatropinDesma ParayuPas encore d'évaluation
- Adverse Drug ReactionsDocument21 pagesAdverse Drug Reactionspharma000100% (1)
- Drug StudyDocument5 pagesDrug StudyGeevine CansinoPas encore d'évaluation
- AntihistaminesDocument49 pagesAntihistaminesKomang Suwarny100% (1)
- Dermatologic PharmacologyDocument88 pagesDermatologic PharmacologyAlunaficha Melody KiraniaPas encore d'évaluation
- Dermatology Supplement v2018 PDFDocument39 pagesDermatology Supplement v2018 PDFVenice Jamaila DagcutanPas encore d'évaluation
- Pharmacology Test 3 Drug ListDocument32 pagesPharmacology Test 3 Drug ListSHRIKANTPas encore d'évaluation
- Drug Therapy in DermatologyDocument486 pagesDrug Therapy in Dermatologyqian88100% (2)
- Initial PE and Labs History Initial Impression: Location &Document1 pageInitial PE and Labs History Initial Impression: Location &kaydee.arPas encore d'évaluation
- Onco PharmacologyDocument9 pagesOnco Pharmacologyarn0ld21Pas encore d'évaluation
- Different Types of Anesthesia and SuturesDocument19 pagesDifferent Types of Anesthesia and SuturesJuana Ablay NabaldePas encore d'évaluation
- ACTIVITY-1 Ryrey-Converted (Recovered)Document6 pagesACTIVITY-1 Ryrey-Converted (Recovered)Janelle Cabida SupnadPas encore d'évaluation
- Dermatologic Pharmacology 1Document7 pagesDermatologic Pharmacology 1Nikko Angelo AlcalaPas encore d'évaluation
- Heavy Bupivacaine 0.5% or Plain Bupivacaine 0.5% Is TheDocument4 pagesHeavy Bupivacaine 0.5% or Plain Bupivacaine 0.5% Is TheRyrey Abraham PacamanaPas encore d'évaluation
- Routes of AdministrationDocument1 pageRoutes of AdministrationkitabunPas encore d'évaluation
- Beecroft 2010 KDocument3 pagesBeecroft 2010 KCati JurcaPas encore d'évaluation
- Water-Soluble Vitamins Vitamin B Description Importance/Indication Effect of Excessive/Deficiency Amount Sources B 1Document7 pagesWater-Soluble Vitamins Vitamin B Description Importance/Indication Effect of Excessive/Deficiency Amount Sources B 1Ron OlegarioPas encore d'évaluation
- Factors Affecting Democracy in The PhilippinesDocument3 pagesFactors Affecting Democracy in The PhilippinesRon Olegario100% (1)
- Cold Cream USPDocument4 pagesCold Cream USPRon OlegarioPas encore d'évaluation
- Drug Extraction and PhytochemistryDocument2 pagesDrug Extraction and PhytochemistryRon OlegarioPas encore d'évaluation
- Carbohydrate-Containing ProductsDocument5 pagesCarbohydrate-Containing ProductsRon OlegarioPas encore d'évaluation
- Frog's Muscular SystemDocument9 pagesFrog's Muscular SystemRon Olegario95% (22)
- Resume Hi Bar A ZackDocument1 pageResume Hi Bar A ZackAsma AlkuwariPas encore d'évaluation
- Case Analysis SchizoDocument4 pagesCase Analysis SchizoiamELHIZAPas encore d'évaluation
- Presented By: Aprindo Donatus Consultant: Dr. Iqbal Lahmadi, SP - PDDocument13 pagesPresented By: Aprindo Donatus Consultant: Dr. Iqbal Lahmadi, SP - PDAprindoDonatusPas encore d'évaluation
- Richard Belli WorkshopDocument62 pagesRichard Belli WorkshopalicefreespiritPas encore d'évaluation
- The Cervical & Thoracic Spine - Mechanical Diagnosis & Therapy - Vol 2Document288 pagesThe Cervical & Thoracic Spine - Mechanical Diagnosis & Therapy - Vol 2booksbearreading100% (6)
- Ravys ResumeDocument2 pagesRavys Resumeapi-332460214Pas encore d'évaluation
- Respiratory Therapy PresentationDocument11 pagesRespiratory Therapy Presentation003cbty9Pas encore d'évaluation
- NICU Protocol 100Document76 pagesNICU Protocol 100Catherine Lee100% (1)
- Anesthesiology PDFDocument40 pagesAnesthesiology PDFBiswajyoti SahuPas encore d'évaluation
- Shaughnessy Amended ComplaintDocument33 pagesShaughnessy Amended ComplaintthedukechroniclePas encore d'évaluation
- Applying The Four Principles of BioEthicsDocument3 pagesApplying The Four Principles of BioEthicsAurelia Pinder100% (1)
- Core Curriculum For The Dialysis Nurse - Module 1Document7 pagesCore Curriculum For The Dialysis Nurse - Module 1green_archerPas encore d'évaluation
- Fabry DiseaseDocument63 pagesFabry DiseaseKunal PaulPas encore d'évaluation
- Module 2Document2 pagesModule 2Duchess Juliane Jose MirambelPas encore d'évaluation
- ABC of DiabetesDocument111 pagesABC of DiabetesCandy E Ri ViPas encore d'évaluation
- Health Problems MyselfDocument54 pagesHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Head Nursing ToolDocument26 pagesHead Nursing ToolJeneva L. LauzonPas encore d'évaluation
- Comp Predictor Quizlet Study GuideDocument20 pagesComp Predictor Quizlet Study GuideJennifer Vicioso100% (9)
- Acute Kidney InjuryDocument8 pagesAcute Kidney InjuryAchmadNuryadiPas encore d'évaluation
- MedStart UMAT Sample and Practice QuestionsDocument55 pagesMedStart UMAT Sample and Practice QuestionsLyn JiangPas encore d'évaluation
- Stratification in The Cox Model: Patrick BrehenyDocument20 pagesStratification in The Cox Model: Patrick BrehenyRaiJúniorPas encore d'évaluation
- MS 21Document10 pagesMS 21karenkaren09Pas encore d'évaluation
- Drug Overdose: Dr. Diah Ari Safitri, SPPDDocument9 pagesDrug Overdose: Dr. Diah Ari Safitri, SPPDmkafabillahPas encore d'évaluation
- Clinical Biochemistry Past PaperDocument7 pagesClinical Biochemistry Past PaperAnonymous WkIfo0P100% (1)
- Fundamentals of Nursing ReviewerDocument28 pagesFundamentals of Nursing ReviewerJamaica Manuel Iglesias100% (1)
- Special - NCLEX - Exam - Jakarta - Students - PDF Filename UTF-8''Special NCLEX Exam - Jakarta StudentsDocument23 pagesSpecial - NCLEX - Exam - Jakarta - Students - PDF Filename UTF-8''Special NCLEX Exam - Jakarta Studentsrizqi100% (1)
- Alveolar OstitisDocument8 pagesAlveolar OstitisAamir BidiwalaPas encore d'évaluation
- Patient Counseling FormDocument2 pagesPatient Counseling FormMarifuddin Hussaini50% (2)
- Lista Clsi-2014 VTKDocument1 pageLista Clsi-2014 VTKMessy ToapantaPas encore d'évaluation