Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Handbook of Continuing Professional Development For The Health IT ProfessionalDocument315 pagesThe Handbook of Continuing Professional Development For The Health IT ProfessionalAloah122346100% (2)
- Mohsen AttiaDocument3 pagesMohsen AttiaAloah122346100% (1)
- Obstetric and Gynecology: A. ColpotomyDocument44 pagesObstetric and Gynecology: A. ColpotomyAloah122346100% (1)
- Contact Dermatitis Concept MapDocument1 pageContact Dermatitis Concept MapAlexeve TabalPas encore d'évaluation
- Review of The Safety of Application of Cosmetic ProductsDocument35 pagesReview of The Safety of Application of Cosmetic ProductsRebek EscutiaPas encore d'évaluation
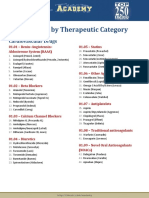
- Drug List by Therapeutic Category: Cardiovascular DrugsDocument7 pagesDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Pas encore d'évaluation
- Part I سنه القمله 2016Document20 pagesPart I سنه القمله 2016Aloah122346Pas encore d'évaluation
- In The Classroom Study Strategies: Better GradesDocument4 pagesIn The Classroom Study Strategies: Better GradesAloah122346100% (1)
- Part ,, Online Contraceptive Related Information Seeking Behaviour QuestionsDocument15 pagesPart ,, Online Contraceptive Related Information Seeking Behaviour QuestionsAloah122346Pas encore d'évaluation
- Saudi Board OSCE2015Document8 pagesSaudi Board OSCE2015Aloah122346Pas encore d'évaluation
- Final Exam Saudi Board 2009Document38 pagesFinal Exam Saudi Board 2009Aloah122346Pas encore d'évaluation
- Saudi Board Exam 2015: These Answers Are Mine, They May Be Right, May Be WrongDocument22 pagesSaudi Board Exam 2015: These Answers Are Mine, They May Be Right, May Be WrongAloah122346Pas encore d'évaluation
- Promotion 2013-2014 With AnswerDocument36 pagesPromotion 2013-2014 With AnswerAloah122346Pas encore d'évaluation
- Workshops, Seminars, Conferences and Symposia Attended During Assistant ProfessorDocument4 pagesWorkshops, Seminars, Conferences and Symposia Attended During Assistant ProfessorAloah122346Pas encore d'évaluation
- Pre NEET Obstetrics and Gynaecology (2013) (PDF) (UnitedVRG)Document320 pagesPre NEET Obstetrics and Gynaecology (2013) (PDF) (UnitedVRG)Aloah122346100% (2)
- 1 PromtionDocument14 pages1 PromtionAloah122346Pas encore d'évaluation
- Promotion OBGYNDocument30 pagesPromotion OBGYNAloah122346Pas encore d'évaluation
- DRTP Specialty Handbook Obstetrics and GynaecologyDocument48 pagesDRTP Specialty Handbook Obstetrics and GynaecologyAloah122346Pas encore d'évaluation
- 2014reVITALizeObstetricDataDefinitionsV10 PDFDocument5 pages2014reVITALizeObstetricDataDefinitionsV10 PDFAloah122346Pas encore d'évaluation
- GTG 36 PDFDocument13 pagesGTG 36 PDFAloah122346Pas encore d'évaluation
- Obesity & It'S Management: Supervised By: Dr. AlnaamiDocument58 pagesObesity & It'S Management: Supervised By: Dr. AlnaamiAloah122346Pas encore d'évaluation
- 25 IcuDocument78 pages25 IcuAloah122346Pas encore d'évaluation
- Ayurskinclinic: Dr. Rohit GoelDocument10 pagesAyurskinclinic: Dr. Rohit GoelPuneet guptaPas encore d'évaluation
- Best Fruits For Hair GrowthDocument19 pagesBest Fruits For Hair Growthfakrul hasanPas encore d'évaluation
- Microblading Aftercare Instructions and ConsentDocument2 pagesMicroblading Aftercare Instructions and ConsentElaine NierrasPas encore d'évaluation
- How To Care For Eczema in Babies and KidsDocument3 pagesHow To Care For Eczema in Babies and KidsTara CamposPas encore d'évaluation
- Nursing Diagnosis For TonsillitisDocument3 pagesNursing Diagnosis For TonsillitisVaneca Go67% (9)
- MD - DVL Q Paper - IDocument8 pagesMD - DVL Q Paper - ISantosh Reddy MandadiPas encore d'évaluation
- Personal IdentificationDocument122 pagesPersonal Identificationkarl luisPas encore d'évaluation
- PowerPoint - Presentation - About - Integumentary - SystemDocument27 pagesPowerPoint - Presentation - About - Integumentary - SystemPrayl Hope NapanoPas encore d'évaluation
- Squamous Cell Carcinoma (SCC) of The SkinDocument17 pagesSquamous Cell Carcinoma (SCC) of The Skinrizka hastariPas encore d'évaluation
- Chapter IV - Dermatology: Common Skin Procedures BiopsyDocument6 pagesChapter IV - Dermatology: Common Skin Procedures BiopsyIndranil SinhaPas encore d'évaluation
- Tongue Conditions: ThrushDocument5 pagesTongue Conditions: ThrushMark TiongsonPas encore d'évaluation
- Res Ipsa Loquitur "The Thing Speaks For Itself"Document14 pagesRes Ipsa Loquitur "The Thing Speaks For Itself"Jay-r Pabualan DacoPas encore d'évaluation
- Retrospective Analysis of The Relationship Between Infantile Seborrheic Dermatitis and Atopic DermatitisDocument6 pagesRetrospective Analysis of The Relationship Between Infantile Seborrheic Dermatitis and Atopic DermatitisIkmal ShahromPas encore d'évaluation
- Derma BriefDocument7 pagesDerma BriefjeharatPas encore d'évaluation
- 10 Best Homeopathic Medicines For AcneDocument13 pages10 Best Homeopathic Medicines For AcneAyeshik ChakrabortyPas encore d'évaluation
- Shivanshu Gangwar M. Pharma (Pharmaceutics)Document16 pagesShivanshu Gangwar M. Pharma (Pharmaceutics)Shibbu GangwarPas encore d'évaluation
- Dermatology Mind MapsDocument39 pagesDermatology Mind MapsRafen NoelPas encore d'évaluation
- Penatalaksanaan Liken Amiloidosis Dengan Desoksimetason Dan Asam Salisilat Topikal: Laporan KasusDocument6 pagesPenatalaksanaan Liken Amiloidosis Dengan Desoksimetason Dan Asam Salisilat Topikal: Laporan KasusmutmainnahPas encore d'évaluation
- LMMJ - Midterms 1.1 - Medico-Legal Aspects of Physical Injuries I TransDocument6 pagesLMMJ - Midterms 1.1 - Medico-Legal Aspects of Physical Injuries I Transchocoholic potchiPas encore d'évaluation
- Medical Surgical Nursing QuizDocument16 pagesMedical Surgical Nursing QuizJohanna Recca MarinoPas encore d'évaluation
- Appearance of A NewbornDocument8 pagesAppearance of A NewbornAlvin U. DumdumaPas encore d'évaluation
- Manuel 6 en 1Document16 pagesManuel 6 en 1Andrea Rios Rojas100% (1)
- Sun SafetyDocument1 pageSun Safetyapi-454487991Pas encore d'évaluation
- Tips To Stay Safe in The SunDocument4 pagesTips To Stay Safe in The Sunsakuraleeshaoran100% (1)
- Topical Steroid Abuse PPT For Family PhysiciansDocument74 pagesTopical Steroid Abuse PPT For Family Physiciansdevsuman sharmaPas encore d'évaluation
- Jangan Di BukaDocument15 pagesJangan Di BukaNuraga Dwi PratapaPas encore d'évaluation
- The Zodiac and The Salts of SalvationDocument32 pagesThe Zodiac and The Salts of Salvationrogerfpa100% (1)
- Dermatoven MCQDocument30 pagesDermatoven MCQS2 GIZI FKUI 2020Pas encore d'évaluation