Vous aimerez peut-être aussi
- Ages and Stages 24 Months QuestionairreDocument8 pagesAges and Stages 24 Months QuestionairreandikaisnaeniPas encore d'évaluation
- 4 Year Questionnaire PDFDocument8 pages4 Year Questionnaire PDFSurabhi Gupta ThakurPas encore d'évaluation
- Asq 5yrsDocument9 pagesAsq 5yrsapi-349363475Pas encore d'évaluation
- Asq 3 8 M PDFDocument7 pagesAsq 3 8 M PDFAnsh AncaPas encore d'évaluation
- Ages and Stages 18 Months QuestionairreDocument7 pagesAges and Stages 18 Months QuestionairreKusuma RamadhaniPas encore d'évaluation
- Asq 3 54 M PDFDocument8 pagesAsq 3 54 M PDFnay nayPas encore d'évaluation
- Month Questionnaire: Ages & Stages QuestionnairesDocument6 pagesMonth Questionnaire: Ages & Stages QuestionnairesDeff HaningPas encore d'évaluation
- ASQ-3 English QuestionnaireDocument6 pagesASQ-3 English QuestionnairetaxidiaraPas encore d'évaluation
- Asq 3 6 M PDFDocument7 pagesAsq 3 6 M PDFnay nayPas encore d'évaluation
- Ages and Stages 9 Months QuestionairreDocument7 pagesAges and Stages 9 Months QuestionairreimuthandchaPas encore d'évaluation
- Month Questionnaire: Ages & Stages QuestionnairesDocument7 pagesMonth Questionnaire: Ages & Stages QuestionnairesamaliakhoirunnisaPas encore d'évaluation
- Month Questionnaire: Ages & Stages QuestionnairesDocument7 pagesMonth Questionnaire: Ages & Stages QuestionnairesAdriane CarqueijoPas encore d'évaluation
- Asq 3 42 MDocument8 pagesAsq 3 42 MMohammed AlsuwaidiPas encore d'évaluation
- Month Questionnaire: Child's NameDocument7 pagesMonth Questionnaire: Child's NameKey KeyPas encore d'évaluation
- Ages Stages Learning Activities 2004Document70 pagesAges Stages Learning Activities 2004GabrielaPanteleouPas encore d'évaluation
- Asq 3 PDFDocument191 pagesAsq 3 PDFAna SantosPas encore d'évaluation
- Early Childhood and Development Checklist 2017 - 2018Document2 pagesEarly Childhood and Development Checklist 2017 - 2018Valen GraylePas encore d'évaluation
- Asq For Parents PacketDocument4 pagesAsq For Parents Packetapi-422038067Pas encore d'évaluation
- The Movment ABC Template For Evaluations AB-2 7-10 YearsDocument2 pagesThe Movment ABC Template For Evaluations AB-2 7-10 YearsFerris100% (1)
- SCREENING - DEVELOPMENTAL DELAY & AUTISM - CCBS DP Infant-Toddler ChecklistDocument9 pagesSCREENING - DEVELOPMENTAL DELAY & AUTISM - CCBS DP Infant-Toddler ChecklistMihaela Grigoroiu100% (1)
- Developmental Delay & Autism Spectrum Disorder Screening ToolsDocument5 pagesDevelopmental Delay & Autism Spectrum Disorder Screening ToolsTanFransisca DianPas encore d'évaluation
- Assessment For Effective Intervention 2002 Rinner 37 46Document11 pagesAssessment For Effective Intervention 2002 Rinner 37 46azrinnePas encore d'évaluation
- User'S Guide User'S Guide: Diane Bricker Joann (JJ) JohnsonDocument32 pagesUser'S Guide User'S Guide: Diane Bricker Joann (JJ) JohnsonPamGarcíaPas encore d'évaluation
- Movement ABC 2 Frequently Asked QuestionsDocument8 pagesMovement ABC 2 Frequently Asked QuestionsCat Graverobber Iskariot0% (1)
- Sensory Profile 2 (SP2) : Age Range: Time To AdministerDocument3 pagesSensory Profile 2 (SP2) : Age Range: Time To Administer宗轶烜Pas encore d'évaluation
- Cuestionarios Inglés ASQ SE 2Document122 pagesCuestionarios Inglés ASQ SE 2María Auxiliadora VasconezPas encore d'évaluation
- Sample Report: Dyslexia Early Screening Test - Second Edition (DEST-2)Document5 pagesSample Report: Dyslexia Early Screening Test - Second Edition (DEST-2)Mudassar HussainPas encore d'évaluation
- PEDS DM Developmental Milestone SurveryDocument1 pagePEDS DM Developmental Milestone SurveryNikolayPas encore d'évaluation
- Child Developmental MilestonesDocument11 pagesChild Developmental MilestonesLassanah KeitaPas encore d'évaluation
- ASQ Master Set PDFDocument100 pagesASQ Master Set PDFКонстантин КрахмалевPas encore d'évaluation
- Ca-Asq-3 EnglishDocument191 pagesCa-Asq-3 Englishapi-301240324100% (1)
- Sample: Sensory Processing Measure-PreschoolDocument1 pageSample: Sensory Processing Measure-PreschoolQORI KARUNIA WANTIPas encore d'évaluation
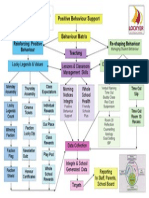
- Positive Behaviour SupportsDocument1 pagePositive Behaviour SupportsCandice BurchPas encore d'évaluation
- Learning Through Play:: A Creative Approach in Teaching Young ChildrenDocument30 pagesLearning Through Play:: A Creative Approach in Teaching Young ChildrenEloisa Arceo ElementoPas encore d'évaluation
- Schon Ell Reading TestDocument1 pageSchon Ell Reading TestGenie SorianoPas encore d'évaluation
- FIRSTSTEPSFIRSTDocument6 pagesFIRSTSTEPSFIRSTcirclestretch100% (1)
- DIR® Assessment: Diane Cullinane, M.D. ICDL Southern California DIR®/Floortime™ Regional Institute 2009-2010Document42 pagesDIR® Assessment: Diane Cullinane, M.D. ICDL Southern California DIR®/Floortime™ Regional Institute 2009-2010circlestretch100% (1)
- Visual Motor Integration WebinarDocument5 pagesVisual Motor Integration WebinarAnonymous QqyLDoW1100% (1)
- CSBSDocument8 pagesCSBSRabia ZubairPas encore d'évaluation
- Interim Devel Assessment Instruments Early InterventionDocument3 pagesInterim Devel Assessment Instruments Early Interventionapi-579880102Pas encore d'évaluation
- s3 Ages and Stages ReportDocument1 pages3 Ages and Stages Reportapi-430374288Pas encore d'évaluation
- BriganceDocument1 pageBriganceamf780% (1)
- IL Early Dev Chart WebDocument4 pagesIL Early Dev Chart WebMuhammad Muzammal HussainPas encore d'évaluation
- PBS Families PDFDocument10 pagesPBS Families PDFCandice Burch100% (1)
- Further Information: ManualDocument44 pagesFurther Information: Manualmina mirPas encore d'évaluation
- Curriculum Curriculum: Beginning BeginningDocument23 pagesCurriculum Curriculum: Beginning BeginningPamGarcíaPas encore d'évaluation
- Critically Appraised Paper For SOS FeedingDocument6 pagesCritically Appraised Paper For SOS FeedingJohn DoePas encore d'évaluation
- Child Devolepment Inventory PDFDocument50 pagesChild Devolepment Inventory PDFSarra Bouslah Ep Bouaouina100% (1)
- Sharing Books With ToddlersDocument3 pagesSharing Books With ToddlersStephanie García EscobarPas encore d'évaluation
- Peabody y Movent ABCDocument11 pagesPeabody y Movent ABCIngrid BarkoPas encore d'évaluation
- Social DevelopmentDocument75 pagesSocial DevelopmentAjay SharmaPas encore d'évaluation
- Abas ModelDocument9 pagesAbas ModelTeodora RusuPas encore d'évaluation
- Sensory Processing FREE Starter Pack PDFDocument31 pagesSensory Processing FREE Starter Pack PDFAnonymous HpNOZkPas encore d'évaluation
- The Efficacy of Sensory Integration Therapy On Children With Asperger's Syndrome and Pdd-NosDocument278 pagesThe Efficacy of Sensory Integration Therapy On Children With Asperger's Syndrome and Pdd-NosAbu FayyadhPas encore d'évaluation
- S3 CARS 2 SampleWriteUp 1Document1 pageS3 CARS 2 SampleWriteUp 1Janet FernandezPas encore d'évaluation
- AutismMotorSkillEvaluationFINALBESt028.8 27 09Document6 pagesAutismMotorSkillEvaluationFINALBESt028.8 27 09Shayne Tee-MelegritoPas encore d'évaluation
- Selected Developmental Screening Tools A Resource For Early EducatorsDocument60 pagesSelected Developmental Screening Tools A Resource For Early EducatorsEva Sala RenauPas encore d'évaluation
- Math - Counting BlocksDocument6 pagesMath - Counting BlocksSurabhi Gupta ThakurPas encore d'évaluation
- Dinosaur CardsDocument8 pagesDinosaur CardsSurabhi Gupta ThakurPas encore d'évaluation
- Shark Matching and Fact CardsDocument5 pagesShark Matching and Fact CardsSurabhi Gupta ThakurPas encore d'évaluation
- Dinosaurs KinderDocument19 pagesDinosaurs KinderSurabhi Gupta ThakurPas encore d'évaluation
- Explode The Code Book 1 Is The First Book in TheDocument10 pagesExplode The Code Book 1 Is The First Book in TheSurabhi Gupta ThakurPas encore d'évaluation
- Examples of Long Vowel Words: With The Long "A" SoundDocument4 pagesExamples of Long Vowel Words: With The Long "A" SoundSurabhi Gupta ThakurPas encore d'évaluation
- BibliographyDocument473 pagesBibliographyMr M100% (2)
- Bajaj Auto Ltd. Business Strategy Case StudyDocument31 pagesBajaj Auto Ltd. Business Strategy Case Studyumangjalan1375% (12)
- Sentinel Event PaperDocument12 pagesSentinel Event Paperapi-285998412Pas encore d'évaluation
- POTANGINADocument18 pagesPOTANGINAJames DapatPas encore d'évaluation
- NASA Confirms People Are Capable of Super Human Abilities Using These Ancient TechniquesDocument4 pagesNASA Confirms People Are Capable of Super Human Abilities Using These Ancient TechniquesIgor Cverdelj-FogarasiPas encore d'évaluation
- Characteristics and Identification of Learners With Hearing NeedsDocument4 pagesCharacteristics and Identification of Learners With Hearing NeedsCarvingBrain.comPas encore d'évaluation
- TarzanDocument25 pagesTarzanMonish BossPas encore d'évaluation
- Disaster From Different PerspectivesDocument20 pagesDisaster From Different PerspectivesJames NanoPas encore d'évaluation
- The Kinslow System Your Path To Proven Success in Health Love and Life PDFDocument20 pagesThe Kinslow System Your Path To Proven Success in Health Love and Life PDFAmy Louise Platt Ferreira0% (5)
- Join The ArmyDocument3 pagesJoin The ArmyJuliet Estud Binay-anPas encore d'évaluation
- 4B Quiz 1 Units 5-6Document3 pages4B Quiz 1 Units 5-6Zuleika ArauzPas encore d'évaluation
- Heartmath Institute Solution For Job StressDocument28 pagesHeartmath Institute Solution For Job StressgafybPas encore d'évaluation
- Adding Two 2-Digit Numbers With Regrouping Lesson PlanDocument3 pagesAdding Two 2-Digit Numbers With Regrouping Lesson Planapi-283422107100% (2)
- ACT-Fundamentos ConceptualesDocument34 pagesACT-Fundamentos ConceptualesLeo Edison C JPas encore d'évaluation
- Buck Institute PBL Planning Form FILLABLEDocument8 pagesBuck Institute PBL Planning Form FILLABLEsaramurrayPas encore d'évaluation
- Lecture 1 (Introduction To HR Analytics)Document53 pagesLecture 1 (Introduction To HR Analytics)Deeksha Singh100% (7)
- Building Consistency Between Title, Problem Statement, Purpose, & Research Questions To Improve The Quality of Research Plans and ReportsDocument10 pagesBuilding Consistency Between Title, Problem Statement, Purpose, & Research Questions To Improve The Quality of Research Plans and ReportssergiocelisjrPas encore d'évaluation
- Reverse SpeechDocument55 pagesReverse Speechramith1100% (2)
- Module 7 Artistic and Creativity LiteracyDocument6 pagesModule 7 Artistic and Creativity LiteracyElla Marie DeñolaPas encore d'évaluation
- Current Trends and Issues in EducationDocument24 pagesCurrent Trends and Issues in EducationJocelyn Sumili100% (1)
- Public Administration Unit-5 Comparative Public AdministrationDocument11 pagesPublic Administration Unit-5 Comparative Public AdministrationDeepika Sharma88% (8)
- P.E Health Lesson PlansDocument5 pagesP.E Health Lesson PlansKendra DoylePas encore d'évaluation
- SM-08-new QQQQDocument41 pagesSM-08-new QQQQpsbacloud100% (1)
- Belbin Team Roles QuestionnaireDocument3 pagesBelbin Team Roles Questionnaireapi-248119294Pas encore d'évaluation
- Sociological Influences On Consumer Decision Making & Cross - Cultural ConsumersDocument19 pagesSociological Influences On Consumer Decision Making & Cross - Cultural ConsumersroshniPas encore d'évaluation
- Check Websites DailywebsitesDocument5 pagesCheck Websites DailywebsitesSup IanPas encore d'évaluation
- Existentialism, Phenomenology and EducationDocument43 pagesExistentialism, Phenomenology and Educationrosminiaisyah0% (1)
- Cajori - The History of Zeno's Arguments On Motion - Phases in The Development of The Theory of LimitsDocument7 pagesCajori - The History of Zeno's Arguments On Motion - Phases in The Development of The Theory of LimitseugenruPas encore d'évaluation
- A Comparative Study of Alienation Among Urban and Rural College Students of Delhi UniversityDocument5 pagesA Comparative Study of Alienation Among Urban and Rural College Students of Delhi UniversityInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Social Effects of The Berlin WallDocument10 pagesSocial Effects of The Berlin WallToriaJ13Pas encore d'évaluation
- The King's SpeechDocument7 pagesThe King's SpeechJo Ann Danao ReyesPas encore d'évaluation
- I Am Sam - EditedDocument4 pagesI Am Sam - EditedBrian ochieng100% (1)