Vous aimerez peut-être aussi
- Project Report On MaleriaDocument50 pagesProject Report On Maleriaasutosh0% (1)
- Mental Health Services in IndiaDocument10 pagesMental Health Services in IndiaMr cholaPas encore d'évaluation
- Dengue Case DiscussionDocument16 pagesDengue Case DiscussionCorinne Fatima de AsisPas encore d'évaluation
- NIBEDITA SAHU-final ThesisDocument78 pagesNIBEDITA SAHU-final ThesisSuman AgrawalPas encore d'évaluation
- IGNOU MSCCFT Block-1Document180 pagesIGNOU MSCCFT Block-1Dr. Megha RichhariyaPas encore d'évaluation
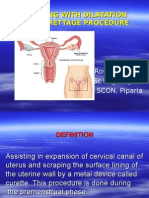
- Assisting With Dilatation and Curettage ProcedureDocument18 pagesAssisting With Dilatation and Curettage ProcedureRoselineTiggaPas encore d'évaluation
- Batch-5 IOT Enabled Air Pollution Monitoring SystemDocument44 pagesBatch-5 IOT Enabled Air Pollution Monitoring SystemSreevani GaddamPas encore d'évaluation
- PROJECTDocument20 pagesPROJECTTechTalkPas encore d'évaluation
- Control of Hospital Acquired Infection PDFDocument36 pagesControl of Hospital Acquired Infection PDFPrakashPas encore d'évaluation
- Project of ThalassemiaDocument10 pagesProject of ThalassemiaOsama ALGabriPas encore d'évaluation
- TUBERCULOSISDocument47 pagesTUBERCULOSISIfeoluwa Deborah Olopade100% (1)
- Visceral Leishmaniasis in IndiaDocument27 pagesVisceral Leishmaniasis in IndiaNishant SrivastavaPas encore d'évaluation
- Communicable Disease Review MaterialDocument43 pagesCommunicable Disease Review Materialrceponelas1127Pas encore d'évaluation
- Tuberculosis Project Report pdf3 PDFDocument35 pagesTuberculosis Project Report pdf3 PDFpari bPas encore d'évaluation
- Epidemiology of Nosocomial Infections (Ncis) Part-1Document42 pagesEpidemiology of Nosocomial Infections (Ncis) Part-1Indah IndrianiPas encore d'évaluation
- 13.format - App-Hand Anthropometry and Grip StrengthDocument6 pages13.format - App-Hand Anthropometry and Grip StrengthImpact JournalsPas encore d'évaluation
- Universal Immunization ProgramDocument15 pagesUniversal Immunization Programsmruti ranjanPas encore d'évaluation
- AIIMS June 2020 - PSM QuestionsDocument7 pagesAIIMS June 2020 - PSM QuestionsadiPas encore d'évaluation
- Immunitization and VaccinationDocument46 pagesImmunitization and VaccinationMazhar RehmanPas encore d'évaluation
- Lesson Plan On Preterm CareDocument4 pagesLesson Plan On Preterm CarePabhat KumarPas encore d'évaluation
- Kap QuestionnaireDocument10 pagesKap QuestionnaireSowmi AnitaPas encore d'évaluation
- Patanjali SWOT AnalysisDocument7 pagesPatanjali SWOT AnalysisDivyajit MahakulPas encore d'évaluation
- Executive Summary: Babasab PatilDocument85 pagesExecutive Summary: Babasab PatilRahil MapariPas encore d'évaluation
- Market Share of Dabur Real JuiceDocument66 pagesMarket Share of Dabur Real Juicesushmit raj badolaPas encore d'évaluation
- Soil Analysis and Agricultural SurveyDocument38 pagesSoil Analysis and Agricultural SurveySarvesh RautPas encore d'évaluation
- Project Augustine AbisolaDocument59 pagesProject Augustine AbisolaRoseline Omoare100% (1)
- MalariaDocument4 pagesMalariaAna May Ramas DelgadoPas encore d'évaluation
- Assessment of Knowledge On Cervical Cancer Among Bangladeshi Women A Hospital Based Cross Sectional StudyDocument6 pagesAssessment of Knowledge On Cervical Cancer Among Bangladeshi Women A Hospital Based Cross Sectional StudySrideviRaviPas encore d'évaluation
- Approach To Renal BiopsyDocument77 pagesApproach To Renal BiopsySandeep Kumar VushikamallaPas encore d'évaluation
- Impact of Agricultural Sector On Indian EconomyDocument17 pagesImpact of Agricultural Sector On Indian EconomyAmit Dandapath100% (6)
- SAANS 2021 Guidance Note - 14102021Document11 pagesSAANS 2021 Guidance Note - 14102021VSG100% (1)
- Malaria KPTIDocument41 pagesMalaria KPTIRahmawati HamudiPas encore d'évaluation
- Current Trends of International Trade in IndiaDocument10 pagesCurrent Trends of International Trade in IndiaponnulakshmiPas encore d'évaluation
- Infectious Disease Outbreak RRM PDFDocument75 pagesInfectious Disease Outbreak RRM PDFmichlsy11Pas encore d'évaluation
- RJ Synopsis Antenna RevisedDocument7 pagesRJ Synopsis Antenna RevisedragvshahPas encore d'évaluation
- Biology Investigatory ProjectDocument15 pagesBiology Investigatory ProjectVikas Ojha69% (16)
- Universal Immunization ProgrammeDocument8 pagesUniversal Immunization ProgrammeNagaraj ReddyPas encore d'évaluation
- Mphil Bio-Chemistry ProjectDocument98 pagesMphil Bio-Chemistry ProjectBalaji Rao NPas encore d'évaluation
- Breathing and Exchange of GasDocument7 pagesBreathing and Exchange of GasParasPas encore d'évaluation
- Biology Project About BacteriaDocument5 pagesBiology Project About BacteriaFadi Diab Tamah100% (3)
- Bachelor of Computer Applications (BCA) : Bca 6 Semester CS-76 Project GuidelinesDocument16 pagesBachelor of Computer Applications (BCA) : Bca 6 Semester CS-76 Project GuidelinesSavyan PvPas encore d'évaluation
- DAY Date: Observation ReportDocument30 pagesDAY Date: Observation ReportPadma priyaPas encore d'évaluation
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- Assignment For Clinical Portfolio Sem 2Document2 pagesAssignment For Clinical Portfolio Sem 2Ketheesaran Lingam0% (1)
- Pollution PPT 090720025050 Phpapp02Document31 pagesPollution PPT 090720025050 Phpapp02anmolPas encore d'évaluation
- Sex-Determination System - WikipediaDocument61 pagesSex-Determination System - WikipediaDeepak maliPas encore d'évaluation
- Communicable Disease Epidemiology and Control PDFDocument2 pagesCommunicable Disease Epidemiology and Control PDFSheilaPas encore d'évaluation
- Occupational Hazards in Health Care ProfessionalsDocument33 pagesOccupational Hazards in Health Care Professionalsdocshirin100% (1)
- Ashish Paliwal Rmncha PDFDocument83 pagesAshish Paliwal Rmncha PDFAshish PaliwalPas encore d'évaluation
- International School of Business & Media: Financial Statement AnalysisDocument4 pagesInternational School of Business & Media: Financial Statement AnalysisDeekshaAjeyPas encore d'évaluation
- Final Research Copy - Backup RepairDocument163 pagesFinal Research Copy - Backup Repair19006 Sahel GamitPas encore d'évaluation
- Full Note On MalariaDocument23 pagesFull Note On MalariaSamuel Obeng100% (2)
- Harshiya ProjectDocument63 pagesHarshiya ProjectHarshiya ChintuPas encore d'évaluation
- There Are Four Types of MalariaDocument5 pagesThere Are Four Types of MalariaSatish GuptaPas encore d'évaluation
- Malaria: Nama: Rismawati NIM: C 111 09 752Document6 pagesMalaria: Nama: Rismawati NIM: C 111 09 752Rismawati AcenkPas encore d'évaluation
- MalariaDocument2 pagesMalariaAinur RohmahPas encore d'évaluation
- What Is Malaria PDFDocument6 pagesWhat Is Malaria PDFtisya f raminPas encore d'évaluation
- Malaria PowerpointDocument19 pagesMalaria PowerpointRhonaJadePas encore d'évaluation
- WHO - MalariaDocument7 pagesWHO - Malariareborn007Pas encore d'évaluation
- Anurag Yadav 12 ADocument12 pagesAnurag Yadav 12 Aabhi yadav ritik yadav7878Pas encore d'évaluation
- Pelletization TechnologyDocument47 pagesPelletization Technologydeepak_143Pas encore d'évaluation
- Hyper TentionDocument38 pagesHyper Tentiondeepak_143Pas encore d'évaluation
- "Azithromycin": Bachelor of PharmacyDocument36 pages"Azithromycin": Bachelor of Pharmacydeepak_143Pas encore d'évaluation
- Fungal Infection: Bachelor of PharmacyDocument40 pagesFungal Infection: Bachelor of Pharmacydeepak_143Pas encore d'évaluation
- Review Article Andrographis PaniculataDocument27 pagesReview Article Andrographis Paniculatadeepak_143Pas encore d'évaluation
- Parential ProductDocument53 pagesParential Productdeepak_143Pas encore d'évaluation
- ChapterDocument11 pagesChapterdeepak_143Pas encore d'évaluation
- Solanum NigrumDocument31 pagesSolanum Nigrumdeepak_143Pas encore d'évaluation
- Cinchona TreeDocument24 pagesCinchona Treedeepak_143Pas encore d'évaluation
- Anti-Inflammatory Drugs: Bachelor of PharmacyDocument37 pagesAnti-Inflammatory Drugs: Bachelor of Pharmacydeepak_1430% (1)
- Herbal DrugDocument33 pagesHerbal Drugdeepak_143Pas encore d'évaluation
- Index: AbstractDocument42 pagesIndex: Abstractdeepak_143Pas encore d'évaluation
- Cinchona DiseaseDocument35 pagesCinchona Diseasedeepak_143Pas encore d'évaluation
- AntiDocument29 pagesAntideepak_143Pas encore d'évaluation
- INTRODUCTION Sunday TypeDocument17 pagesINTRODUCTION Sunday Typedeepak_143Pas encore d'évaluation
- Andrographis PaniculataDocument34 pagesAndrographis Paniculatadeepak_143Pas encore d'évaluation
- Employee Management System: Background StudyDocument71 pagesEmployee Management System: Background Studydeepak_143Pas encore d'évaluation
- Academic ManagmentDocument59 pagesAcademic Managmentdeepak_143Pas encore d'évaluation
- Training Project Report On: "Instrumentation in Cement Plant"Document1 pageTraining Project Report On: "Instrumentation in Cement Plant"deepak_143Pas encore d'évaluation
- Saraswati Science College: A Project Report OnDocument6 pagesSaraswati Science College: A Project Report Ondeepak_143Pas encore d'évaluation
- Academic ManagmentDocument59 pagesAcademic Managmentdeepak_143Pas encore d'évaluation
- Industrial Tranning 01report 2013Document27 pagesIndustrial Tranning 01report 2013deepak_143Pas encore d'évaluation
- No. of Beneficiaries: InterpretationDocument7 pagesNo. of Beneficiaries: Interpretationdeepak_143Pas encore d'évaluation
- Overview of All India RadioDocument28 pagesOverview of All India Radiodeepak_143Pas encore d'évaluation
- Cover PageDocument2 pagesCover Pagedeepak_143Pas encore d'évaluation
- Encypted FileDocument83 pagesEncypted Filedeepak_143Pas encore d'évaluation
- Airline Reservation System Project ReportDocument66 pagesAirline Reservation System Project Reportnasilalap100% (1)
- Airline Reservation System Visual BasicDocument91 pagesAirline Reservation System Visual Basicdeepak_143Pas encore d'évaluation
- File Management SystemDocument83 pagesFile Management Systemdeepak_143Pas encore d'évaluation
- Budget ApprovalDocument102 pagesBudget Approvaldeepak_143Pas encore d'évaluation
- Research Themes and Advances in MalariaDocument11 pagesResearch Themes and Advances in Malarialilibeth paola duran plataPas encore d'évaluation
- MalariaDocument15 pagesMalariaEssa KhanPas encore d'évaluation
- Malaria MCQDocument7 pagesMalaria MCQTony Dawa100% (3)
- Part-2-ParasitologyDocument33 pagesPart-2-ParasitologyAli AhmedPas encore d'évaluation
- MalariaDocument21 pagesMalariayusak tapakedingPas encore d'évaluation
- Pathcare May-Aug PDFDocument6 pagesPathcare May-Aug PDFdenosciPas encore d'évaluation
- MalariaDocument30 pagesMalariaderilPas encore d'évaluation
- Case Studies: Recurrent Fever, Chills, and Malaise in A 53-Year-Old ManDocument2 pagesCase Studies: Recurrent Fever, Chills, and Malaise in A 53-Year-Old Mansreeja maragoniPas encore d'évaluation
- Malaria Rapid Diagnostic Test ProductsDocument39 pagesMalaria Rapid Diagnostic Test ProductsferaayudianovitaPas encore d'évaluation
- Malaria Managment Algorithm 202208Document1 pageMalaria Managment Algorithm 202208Marianne Joy PontigonPas encore d'évaluation
- By: Dr. NG Chean Hui (PHD in Medicinal Chemistry, Upm)Document41 pagesBy: Dr. NG Chean Hui (PHD in Medicinal Chemistry, Upm)Maria Florina100% (1)
- Malaria Journal Malaria JournalDocument20 pagesMalaria Journal Malaria JournalYuda Arie DharmawanPas encore d'évaluation
- 13 - MalariaDocument12 pages13 - MalariaNokiaPas encore d'évaluation
- Epidemiology Prevention & Control of Malaria: Dr. Neha Tyagi Assistant Professor Department of Community MedicineDocument29 pagesEpidemiology Prevention & Control of Malaria: Dr. Neha Tyagi Assistant Professor Department of Community MedicineShashi TyagiPas encore d'évaluation
- Disease Caused by ProtozoansDocument21 pagesDisease Caused by ProtozoansBrijesh KumarPas encore d'évaluation
- اسئله مهمه طفيليات نضريDocument11 pagesاسئله مهمه طفيليات نضريxrmd8khg7rPas encore d'évaluation
- Study Guide of Medical Parasitology, Part 1. ProtozoologyDocument50 pagesStudy Guide of Medical Parasitology, Part 1. Protozoologymicrobehunter007Pas encore d'évaluation
- Bahan CA 1Document11 pagesBahan CA 1fk unswagatiPas encore d'évaluation
- Another DedicationDocument21 pagesAnother DedicationFarida AdiningrumPas encore d'évaluation
- Biological Activities of Lupeol DesecurizatOKDocument21 pagesBiological Activities of Lupeol DesecurizatOKLiviu Athos TamasPas encore d'évaluation
- MalariaDocument28 pagesMalariaArthur Samuel ShavaniPas encore d'évaluation
- Malaria Case PresentationDocument36 pagesMalaria Case Presentationkamal_zaidi04Pas encore d'évaluation
- Malaria EpidemicDocument49 pagesMalaria EpidemicB BCPas encore d'évaluation
- Malaria and Climate Change1248scribdDocument3 pagesMalaria and Climate Change1248scribdGuadalupe JamesPas encore d'évaluation
- An Introduction of MalariaDocument19 pagesAn Introduction of MalariaSomesh GuptaPas encore d'évaluation
- GRP 04 Clin paraDocument47 pagesGRP 04 Clin paraJeddhie MoraPas encore d'évaluation
- Expertreview AtharDocument22 pagesExpertreview AtharayuPas encore d'évaluation
- E. Histolytica Trophozoites Secrete Cysteine Proteases WhichDocument16 pagesE. Histolytica Trophozoites Secrete Cysteine Proteases WhichAherrera BanzuelaPas encore d'évaluation
- Plantas EndemicasDocument17 pagesPlantas EndemicasAdilson Notório VeigaPas encore d'évaluation
- Lab Exercises in ParasitologyDocument8 pagesLab Exercises in ParasitologyNinaRicaR.Ramos0% (1)