Vous aimerez peut-être aussi
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Port of ManilaDocument29 pagesPort of ManilaPrecious Mae Saguid Sager75% (4)
- Management Control System: Presentation TopicDocument16 pagesManagement Control System: Presentation TopicVj AutiPas encore d'évaluation
- Project EvaluationDocument4 pagesProject EvaluationUkesh ShresthaPas encore d'évaluation
- Hygienic Chappathi Business Loan ReportDocument13 pagesHygienic Chappathi Business Loan ReportJose PiusPas encore d'évaluation
- Finals Quiz #2 Soce, Soci, Ahfs and Do Multiple Choice: Account Title AmountDocument3 pagesFinals Quiz #2 Soce, Soci, Ahfs and Do Multiple Choice: Account Title AmountNew TonPas encore d'évaluation
- 1.4 Planning and Structuring The Cost Audit 1.4.1 Need For Planning An AuditDocument5 pages1.4 Planning and Structuring The Cost Audit 1.4.1 Need For Planning An AuditAnu Yashpal KapoorPas encore d'évaluation
- Supply Chain-Case Study of DellDocument3 pagesSupply Chain-Case Study of DellSafijo Alphons100% (1)
- Financing Methods For Import of Capital Goods in IndiaDocument13 pagesFinancing Methods For Import of Capital Goods in IndiaAneesha KasimPas encore d'évaluation
- To Lease or Not To Lease?: Hotel ContractsDocument10 pagesTo Lease or Not To Lease?: Hotel ContractsDaryl ChengPas encore d'évaluation
- Quality Improvement With Statistical Process Control in The Automotive IndustryDocument8 pagesQuality Improvement With Statistical Process Control in The Automotive Industryonii96Pas encore d'évaluation
- E-Business Tax Application SetupDocument25 pagesE-Business Tax Application Setuprasemahe4100% (1)
- Irfz 24 NDocument9 pagesIrfz 24 Njmbernal7487886Pas encore d'évaluation
- Flydubai Menu Issue 09Document11 pagesFlydubai Menu Issue 09Swamy RakeshPas encore d'évaluation
- Case of HyfluxDocument6 pagesCase of HyfluxMai NganPas encore d'évaluation
- Cash Inflow and OutflowDocument6 pagesCash Inflow and OutflowMubeenPas encore d'évaluation
- Topic 4 - Adjusting Accounts and Preparing Financial StatementsDocument18 pagesTopic 4 - Adjusting Accounts and Preparing Financial Statementsapi-388504348100% (1)
- Cash Forecasting For ClassDocument24 pagesCash Forecasting For ClassShaikh Saifullah KhalidPas encore d'évaluation
- Ravikumar S: Specialties: Pre-Opening, Procurement, Implementing Best Practices, Budgets, CostDocument2 pagesRavikumar S: Specialties: Pre-Opening, Procurement, Implementing Best Practices, Budgets, CostMurthy BanagarPas encore d'évaluation
- E-Challan CCMT ChallanDocument2 pagesE-Challan CCMT ChallanSingh KDPas encore d'évaluation
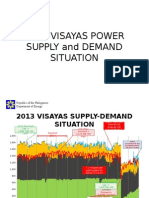
- 2013 Visayas Power Supply and Demand Situation: Republic of The Philippines Department of EnergyDocument10 pages2013 Visayas Power Supply and Demand Situation: Republic of The Philippines Department of EnergyJannet MalezaPas encore d'évaluation
- c19b - Cash Flow To Equity - ModelDocument6 pagesc19b - Cash Flow To Equity - ModelaluiscgPas encore d'évaluation
- Chapter 4 Transportation and Assignment ModelsDocument88 pagesChapter 4 Transportation and Assignment ModelsSyaz Amri100% (1)
- Irf 3205 HexfetDocument12 pagesIrf 3205 Hexfetconti51Pas encore d'évaluation
- Hygeia International: I. Title of The CaseDocument7 pagesHygeia International: I. Title of The CaseDan GabonPas encore d'évaluation
- Bill of Lading: Cable: CSHKAC Telex: 87986 CSHKAHX Port-to-Port or Combined TransportDocument1 pageBill of Lading: Cable: CSHKAC Telex: 87986 CSHKAHX Port-to-Port or Combined TransportMoineePas encore d'évaluation
- AU Small Finance Bank LTD.: General OverviewDocument3 pagesAU Small Finance Bank LTD.: General Overviewdarshan jainPas encore d'évaluation
- How To Attack The Leader - FinalDocument14 pagesHow To Attack The Leader - Finalbalakk06Pas encore d'évaluation
- Chiffon Camisole and Tap Pants PDFDocument34 pagesChiffon Camisole and Tap Pants PDFpiano lov100% (3)
- CompleteDocument2 pagesCompleteappledeja7829Pas encore d'évaluation
- Class 17 - Dabhol Case Study PDFDocument28 pagesClass 17 - Dabhol Case Study PDFBaljeetSinghKhoslaPas encore d'évaluation