Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- New Newstart 2Document1 pageNew Newstart 2Adrian KhomanPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Jae 201174012905Document5 pagesJae 201174012905Adrian KhomanPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Fetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignDocument8 pagesFetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignAdrian KhomanPas encore d'évaluation
- Diagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenDocument7 pagesDiagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenAdrian KhomanPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Pediatric Cardiology: Original ArticlesDocument5 pagesPediatric Cardiology: Original ArticlesAdrian KhomanPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Pocket Pediatric Hematologi OnkologiDocument5 pagesPocket Pediatric Hematologi OnkologiAdrian KhomanPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Miaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoDocument1 pageMiaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoAdrian KhomanPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Pediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDDocument6 pagesPediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDAdrian KhomanPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Hemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Document9 pagesHemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Adrian KhomanPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesDocument8 pagesBreastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesAdrian KhomanPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
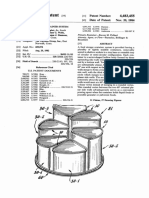
- United States Patent (19) : Prophet, Jr. Et AlDocument13 pagesUnited States Patent (19) : Prophet, Jr. Et AlAdrian KhomanPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 pagesUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Tonkic Et Al 2012 HelicobacterDocument8 pagesTonkic Et Al 2012 HelicobacterAdrian KhomanPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Haemophilus Parainfluenzae Antigen and Antibody in Children: With Iga Nephropathy and Henoch-Scho Nlein NephritisDocument6 pagesHaemophilus Parainfluenzae Antigen and Antibody in Children: With Iga Nephropathy and Henoch-Scho Nlein NephritisAdrian KhomanPas encore d'évaluation
- Reentry Tachycardia in Children: Llustrative ASEDocument4 pagesReentry Tachycardia in Children: Llustrative ASEAdrian KhomanPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Brief: Henoch-Schönlein PurpuraDocument5 pagesBrief: Henoch-Schönlein PurpuraAdrian KhomanPas encore d'évaluation
- NDT 12 1795 PDFDocument13 pagesNDT 12 1795 PDFAdrian KhomanPas encore d'évaluation
- The Oral Microbiome in Health and Disease: Pharmacological ResearchDocument7 pagesThe Oral Microbiome in Health and Disease: Pharmacological ResearchAdrian KhomanPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- RCCM 201406-1049ocDocument8 pagesRCCM 201406-1049ocAdrian KhomanPas encore d'évaluation
- 10 1111@dmcn 12922Document8 pages10 1111@dmcn 12922Adrian KhomanPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Iron Deficiency Anemia (Ida)Document30 pagesIron Deficiency Anemia (Ida)angel214Pas encore d'évaluation
- Anemia Pathophysiology All in 1 by Francis OliverosDocument3 pagesAnemia Pathophysiology All in 1 by Francis Oliverosfrancis00090Pas encore d'évaluation
- Haem Lecture 2.2016 PDFDocument12 pagesHaem Lecture 2.2016 PDFdorsa koraeiPas encore d'évaluation
- Anaphy ReviewerDocument102 pagesAnaphy Reviewermaureensolano63Pas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hematopathology All LecturesDocument226 pagesHematopathology All LecturesYousif AlaaPas encore d'évaluation
- Relationship of Cell-Free Hemoglobin To Impaired Endothelial Nitric Oxide Bioavailability and Perfusion in Severe Falciparum MalariaDocument8 pagesRelationship of Cell-Free Hemoglobin To Impaired Endothelial Nitric Oxide Bioavailability and Perfusion in Severe Falciparum MalariaAhmad ThotuchingPas encore d'évaluation
- Live Blood Atlas PDFDocument9 pagesLive Blood Atlas PDFHadriawan Alimuddin100% (5)
- Blood and Blood ProductsDocument52 pagesBlood and Blood Productswellawalalasith100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Clinical MicrosDocument54 pagesClinical MicrosLois DaniellePas encore d'évaluation
- AnemiaDocument63 pagesAnemiaShyam RajPas encore d'évaluation
- Automation in Haematology - BernardDocument60 pagesAutomation in Haematology - BernardBosco Mbonimpa100% (1)
- Artificial Cells: Life Is Endowed With A Mysterious and Divine Life-ForceDocument52 pagesArtificial Cells: Life Is Endowed With A Mysterious and Divine Life-ForcemissuedPas encore d'évaluation
- Case Scenerio GlomerulonephritisDocument4 pagesCase Scenerio GlomerulonephritisEllen AngelPas encore d'évaluation
- Nursing Care PlanDocument5 pagesNursing Care PlanHikaru TakishimaPas encore d'évaluation
- Topics of This Lecture: RBC: - Structural Characteristics - Hemoglobin - Erythropoiesis - Erythrocytes DestructionDocument23 pagesTopics of This Lecture: RBC: - Structural Characteristics - Hemoglobin - Erythropoiesis - Erythrocytes DestructionHashim GhazoPas encore d'évaluation
- SHS - Biology 1 - Q1 - Module 3 - Reviewed - EditedDocument30 pagesSHS - Biology 1 - Q1 - Module 3 - Reviewed - EditedLiberty Salazar100% (2)
- Anemia: Shannen Kate N. Tercenio PM401Document22 pagesAnemia: Shannen Kate N. Tercenio PM401Shannen Kate TercenioPas encore d'évaluation
- Blood Banking - System RequirementsDocument24 pagesBlood Banking - System RequirementsJira Jinn ChuaPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Regulation of ErythropoiesisDocument3 pagesRegulation of ErythropoiesisFlowerPas encore d'évaluation
- 3B Paper Breakdown UpdatedDocument7 pages3B Paper Breakdown UpdatedNosh AnbreenPas encore d'évaluation
- Clinical For PracticalDocument72 pagesClinical For PracticalYogendra SinghPas encore d'évaluation
- 11m.routine Lab Eval of RBCDocument15 pages11m.routine Lab Eval of RBCella SyPas encore d'évaluation
- Ascp StudyDocument18 pagesAscp StudyJamaica EstorninosPas encore d'évaluation
- Heamtology Reviewer (Midterm)Document15 pagesHeamtology Reviewer (Midterm)Johney DoePas encore d'évaluation
- Hematology NotesDocument24 pagesHematology Notesddrei13Pas encore d'évaluation
- First Grading VIDocument82 pagesFirst Grading VIIvy Villanueva Divino100% (1)
- Organisation of The Organism QPDocument11 pagesOrganisation of The Organism QPViviana PlacentinoPas encore d'évaluation
- HematologyonprobioticsDocument7 pagesHematologyonprobioticsMirela CrețuPas encore d'évaluation
- Biochem Lab NotesDocument5 pagesBiochem Lab NotesSofiaRodriguezPas encore d'évaluation
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (30)