Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Biocompatibility of Dental Materials: DR Khushboo R I MdsDocument113 pagesBiocompatibility of Dental Materials: DR Khushboo R I MdsMV PratyushaPas encore d'évaluation
- 08 - Endodontic Microflora A Review PDFDocument6 pages08 - Endodontic Microflora A Review PDFMV PratyushaPas encore d'évaluation
- Current Developments in Transport Media For Avulsed Teeth: An UpdateDocument4 pagesCurrent Developments in Transport Media For Avulsed Teeth: An UpdateMV PratyushaPas encore d'évaluation
- An in Vivo Technique For Biocompatibility Studies of MaterialsDocument2 pagesAn in Vivo Technique For Biocompatibility Studies of MaterialsMV PratyushaPas encore d'évaluation
- 10 3109@00016357109026512Document8 pages10 3109@00016357109026512MV PratyushaPas encore d'évaluation
- 2 3 5.1Document4 pages2 3 5.1MV PratyushaPas encore d'évaluation
- Click Here To View Optimized Website For Mobile DevicesDocument13 pagesClick Here To View Optimized Website For Mobile DevicesMV PratyushaPas encore d'évaluation
- Presented By: Dr. M V PratyushaDocument23 pagesPresented By: Dr. M V PratyushaMV PratyushaPas encore d'évaluation
- The Effect of Saliva On Dental Caries: JADA 2008 139 (5 Suppl) :11S-17SDocument7 pagesThe Effect of Saliva On Dental Caries: JADA 2008 139 (5 Suppl) :11S-17SMV PratyushaPas encore d'évaluation
- Sim Ezo 2017Document6 pagesSim Ezo 2017MV PratyushaPas encore d'évaluation
- Walmsley 1988Document8 pagesWalmsley 1988MV PratyushaPas encore d'évaluation
- The Effect of Saliva On Dental Caries: JADA 2008 139 (5 Suppl) :11S-17SDocument7 pagesThe Effect of Saliva On Dental Caries: JADA 2008 139 (5 Suppl) :11S-17SMV PratyushaPas encore d'évaluation
- Composites EraDocument235 pagesComposites EraMV PratyushaPas encore d'évaluation
- 2 3 5.1Document4 pages2 3 5.1MV PratyushaPas encore d'évaluation
- Pulp Response To Temporary Restorative MaterialsDocument7 pagesPulp Response To Temporary Restorative MaterialsMV PratyushaPas encore d'évaluation
- Indirect RestorationsDocument13 pagesIndirect RestorationsMV PratyushaPas encore d'évaluation
- Oral Presentations HandoutDocument5 pagesOral Presentations HandoutNikki M. ArapolPas encore d'évaluation
- 08 - Endodontic Microflora A ReviewDocument6 pages08 - Endodontic Microflora A ReviewMV PratyushaPas encore d'évaluation
- Oral Presentations HandoutDocument5 pagesOral Presentations HandoutNikki M. ArapolPas encore d'évaluation
- The Top Advances in Caries Detection - Dental Products Report PDFDocument4 pagesThe Top Advances in Caries Detection - Dental Products Report PDFMV PratyushaPas encore d'évaluation
- Sharpening Dental Hand Instruments: Brook A. Niemiec, DVMDocument3 pagesSharpening Dental Hand Instruments: Brook A. Niemiec, DVMMV PratyushaPas encore d'évaluation
- Indirect RestorationsDocument13 pagesIndirect RestorationsMV PratyushaPas encore d'évaluation
- The Glossary of Prosthodontic Terms 2005 (GPT 8°)Document83 pagesThe Glossary of Prosthodontic Terms 2005 (GPT 8°)pedrali7150% (2)
- Indirect RestorationsDocument13 pagesIndirect RestorationsMV PratyushaPas encore d'évaluation
- Summit V Summary DR Senia by Rob KaufmanDocument5 pagesSummit V Summary DR Senia by Rob KaufmanMV PratyushaPas encore d'évaluation
- Stainless Steel TypesDocument4 pagesStainless Steel TypesMV PratyushaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hierarchy ExampleDocument18 pagesHierarchy ExampleSanket SahuPas encore d'évaluation
- All CompleteDocument10 pagesAll CompleteNanep NanenanenaPas encore d'évaluation
- Gen. Zoo. Final ReviewerDocument34 pagesGen. Zoo. Final ReviewerAshley FranciscoPas encore d'évaluation
- RPT SC Year 2 (DLP) 2022-2023Document21 pagesRPT SC Year 2 (DLP) 2022-2023ANNIE MARGARET A/P ANTHONY MoePas encore d'évaluation
- Contoh Arsitektur SimbioisisDocument12 pagesContoh Arsitektur SimbioisisDeni AtahillahPas encore d'évaluation
- Escueoloside A2 From TomatoDocument8 pagesEscueoloside A2 From TomatoShyam ReddyPas encore d'évaluation
- Determination of Formaldehyde in Tofu From Ciputat Traditional Market With Colorimetry MethodDocument6 pagesDetermination of Formaldehyde in Tofu From Ciputat Traditional Market With Colorimetry Methodhali taekookPas encore d'évaluation
- 16S RRNA Gene Sequencing For Bacterial IdentificationDocument4 pages16S RRNA Gene Sequencing For Bacterial IdentificationBenjamin UcichPas encore d'évaluation
- Life Span: HumanDocument738 pagesLife Span: HumanWAJEEHA GOHARPas encore d'évaluation
- 2023 Wisent Pricing AlbertaDocument7 pages2023 Wisent Pricing Albertavetman8842Pas encore d'évaluation
- 8610 - 1 Maham AslamDocument21 pages8610 - 1 Maham AslamMuhammad BasitPas encore d'évaluation
- Third Stage Begg MechanotherapyDocument32 pagesThird Stage Begg MechanotherapyNaziya ShaikPas encore d'évaluation
- Human Genetics Concepts and Applications 11Th Edition Ricki Lewis Test Bank Full Chapter PDFDocument36 pagesHuman Genetics Concepts and Applications 11Th Edition Ricki Lewis Test Bank Full Chapter PDFdavid.cordero230100% (14)
- Recent DevelopmentsDocument295 pagesRecent DevelopmentsGabriel PinheiroPas encore d'évaluation
- Preparation of Histological SpecimensDocument4 pagesPreparation of Histological SpecimensAqilah HazwaniPas encore d'évaluation
- EASL 2021 Version 4 NewDocument691 pagesEASL 2021 Version 4 NewGupse Köroğlu AdalıPas encore d'évaluation
- Approved LaboratoriesDocument22 pagesApproved LaboratoriesPaul CPas encore d'évaluation
- On The Nature of The Symbiotic Man in Joël de RosnayDocument12 pagesOn The Nature of The Symbiotic Man in Joël de RosnayAJHSSR JournalPas encore d'évaluation
- Dihybrid Punnett SquaresDocument4 pagesDihybrid Punnett SquaresThomas Abich100% (1)
- This Study Resource Was: Your Results 5/5Document5 pagesThis Study Resource Was: Your Results 5/5Pearl PascuaPas encore d'évaluation
- Using STADEN For Sequence AssemblyDocument5 pagesUsing STADEN For Sequence AssemblyChristen Rune StensvoldPas encore d'évaluation
- 7 Pearson SquareDocument19 pages7 Pearson Squareapi-235944649Pas encore d'évaluation
- Instant Download Business Communication 16th Edition Lehman Test Bank PDF Full ChapterDocument32 pagesInstant Download Business Communication 16th Edition Lehman Test Bank PDF Full Chapterarthrosisretake8hro100% (8)
- "Material Ecocriticism and The Creativity of Storied Matter" by Serpil OppermannDocument16 pages"Material Ecocriticism and The Creativity of Storied Matter" by Serpil OppermannoppermanPas encore d'évaluation
- Composite Fish Culture in PondsDocument2 pagesComposite Fish Culture in Pondsvikasdevre1Pas encore d'évaluation
- L&M ResearchDocument145 pagesL&M ResearchJulia PurperaPas encore d'évaluation
- Study Guide Cardio Tayang by Gextha 30 Maret 2015Document82 pagesStudy Guide Cardio Tayang by Gextha 30 Maret 2015Adi ParamarthaPas encore d'évaluation
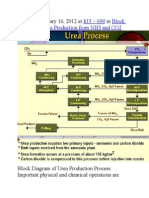
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Document9 pagesPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654Pas encore d'évaluation
- đề thi hsg 12 cấp trường LTK 23-24 - KEYSDocument6 pagesđề thi hsg 12 cấp trường LTK 23-24 - KEYShan nguyenPas encore d'évaluation
- Cham PowerpointDocument19 pagesCham PowerpointElizabeth GenotivaPas encore d'évaluation