Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Biodecoding Total BiologyDocument7 pagesBiodecoding Total Biologygrailfinder75% (4)
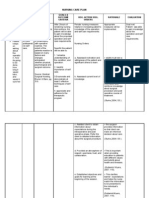
- NSG CARE PLAN FOR AdhdDocument3 pagesNSG CARE PLAN FOR AdhdParuo PatelPas encore d'évaluation
- Child Psychiatric EmergenciesDocument8 pagesChild Psychiatric EmergenciesDanitza YhovannaPas encore d'évaluation
- STSurg NumntDocument11 pagesSTSurg NumntrohiPas encore d'évaluation
- Reflection On Feeding Elderly ClientsDocument2 pagesReflection On Feeding Elderly ClientsLaydee GiaAmPas encore d'évaluation
- Guinea Pigs PDFDocument1 pageGuinea Pigs PDFYaserAbbasiPas encore d'évaluation
- Foods That Kill CandidaDocument3 pagesFoods That Kill Candidasexy_rusian100% (1)
- Swyer James MacLeod SyndromeDocument12 pagesSwyer James MacLeod Syndromeflori.bPas encore d'évaluation
- Dutch COPD Physiotherapy Guidelines PDFDocument64 pagesDutch COPD Physiotherapy Guidelines PDFyohanPas encore d'évaluation
- Quick Reference Guide-04Dec2019Document46 pagesQuick Reference Guide-04Dec2019adiangriawanPas encore d'évaluation
- Gross Motor Development 6to12yearsDocument17 pagesGross Motor Development 6to12yearsGul RockzzPas encore d'évaluation
- Heavy HandsDocument8 pagesHeavy HandsPicklehead McSpazatronPas encore d'évaluation
- Gynecological LaparosDocument32 pagesGynecological LaparosYosef Dwi Cahyadi Salan100% (1)
- MSDS - SiliconeFluid200 350Document7 pagesMSDS - SiliconeFluid200 350Rafael Saldanha LopesPas encore d'évaluation
- Crown LengtheningDocument4 pagesCrown LengtheningArdelvie YoandaPas encore d'évaluation
- POLK COUNTY - Goodrich ISD - 2008 Texas School Survey of Drug and Alcohol UseDocument48 pagesPOLK COUNTY - Goodrich ISD - 2008 Texas School Survey of Drug and Alcohol UseTexas School Survey of Drug and Alcohol UsePas encore d'évaluation
- Clasificare Carii Dentare Otr Cariologie An IIIDocument79 pagesClasificare Carii Dentare Otr Cariologie An IIIStefana NanuPas encore d'évaluation
- Ethics and Patient SafetyDocument10 pagesEthics and Patient SafetyIdeas InfinitePas encore d'évaluation
- NCP 1Document4 pagesNCP 1Ke EjiePas encore d'évaluation
- Enraf-Nonius Manumed Exercise enDocument6 pagesEnraf-Nonius Manumed Exercise enjoseprudencio8848Pas encore d'évaluation
- NCD Guidelines 2012Document12 pagesNCD Guidelines 2012Nari BurathiPas encore d'évaluation
- Chap.30 Complications From Heart Disease WordDocument6 pagesChap.30 Complications From Heart Disease WordcaisakiPas encore d'évaluation
- Oral Rehydration SaltDocument3 pagesOral Rehydration SaltVincent ManganaanPas encore d'évaluation
- Rumah Sakit Bhakti MuliaDocument3 pagesRumah Sakit Bhakti MuliaSarachanda SallyPas encore d'évaluation
- Pain Management NCLEXDocument5 pagesPain Management NCLEXPotchiee PfizerPas encore d'évaluation
- Planning Physical Facilities of Hospital and Educational InstitutionDocument5 pagesPlanning Physical Facilities of Hospital and Educational InstitutionSundaraBharathi100% (2)
- BARC TrainingDocument6 pagesBARC Trainingashfaqk100% (1)
- Combined Cellulitis - FinalDocument78 pagesCombined Cellulitis - Finalsaru_patel0% (1)
- Night FeverDocument5 pagesNight FeverdewioktaPas encore d'évaluation
- Presentation On STP (SBR)Document8 pagesPresentation On STP (SBR)Leo VictorPas encore d'évaluation