Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Changes in Appearance in The Presence of Major Stress EventsDocument8 pagesChanges in Appearance in The Presence of Major Stress EventsPatPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Scimagojr 2020Document2 453 pagesScimagojr 2020heinz billPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- BET 4108-Educational Technology - CAT 1 and 2Document6 pagesBET 4108-Educational Technology - CAT 1 and 2Elias BonkePas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Bodynamic Character Analysis GuideDocument22 pagesBodynamic Character Analysis GuideClara Marina Galliez100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Differential Diagnoses of SeizuresDocument6 pagesDifferential Diagnoses of SeizureslinevetPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Oosthuizen ...Document12 pagesOosthuizen ...JamesPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Michael Hall - Secrets of Personal Mastery (NLP)Document5 pagesMichael Hall - Secrets of Personal Mastery (NLP)swetalogin0% (1)
- Cognitive Therapy Versus Medication - For Depression - Treatment Outcomes - and Neural MechanismsDocument9 pagesCognitive Therapy Versus Medication - For Depression - Treatment Outcomes - and Neural MechanismsComercial 03Pas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Psychology Learning Objectives: - Nervous SystemDocument11 pagesPsychology Learning Objectives: - Nervous SystemjaninePas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- TMP E946Document7 pagesTMP E946FrontiersPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Highly Religious Participants Recruit Areas of Social Cognition in Personal PrayerDocument9 pagesHighly Religious Participants Recruit Areas of Social Cognition in Personal PrayerIgor KhedePas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Diagnostic and Statistical Manual of Mental DisordersDocument16 pagesDiagnostic and Statistical Manual of Mental DisordersKen MurrayPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Coek - Info - Neurocomputing Foundations of ResearchDocument5 pagesCoek - Info - Neurocomputing Foundations of Researchkgdeepak122950Pas encore d'évaluation
- UntitledDocument2 pagesUntitledAsad RzayevPas encore d'évaluation
- A Guide To Introduce Literature in The English Language ClassDocument5 pagesA Guide To Introduce Literature in The English Language ClassRosalina RodríguezPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Neurocare TMS-application enDocument28 pagesNeurocare TMS-application enRaluca ComanescuPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Counseling Teenagers: Perspective On CounsellingDocument21 pagesCounseling Teenagers: Perspective On CounsellingparlinpurbaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- How Emotional Intelligence Became A Key Leadership Skill: What To Read NextDocument12 pagesHow Emotional Intelligence Became A Key Leadership Skill: What To Read NextSintya RistriyaniPas encore d'évaluation
- Neural Control and Coordination (Edustudy Point) - UnlockedDocument8 pagesNeural Control and Coordination (Edustudy Point) - Unlockedkushwahvivek1028Pas encore d'évaluation
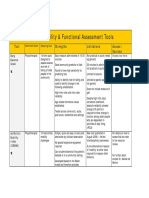
- 2013 Table 1 Mobility and Functional Assessment Tools PDFDocument4 pages2013 Table 1 Mobility and Functional Assessment Tools PDFesbat07Pas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Shallows PDFDocument6 pagesThe Shallows PDFRamona Padurean67% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- RRLDocument3 pagesRRLJiffy Roseveery CervantesPas encore d'évaluation
- Philosophy of Artificial IntelligenceDocument52 pagesPhilosophy of Artificial Intelligenceetitah100% (4)
- Abnormal Psychology in A Changing World (9th Edition)Document657 pagesAbnormal Psychology in A Changing World (9th Edition)Ken Oceana50% (6)
- AttractionDocument6 pagesAttractionElena-Andreea MutPas encore d'évaluation
- Kod DeduktifDocument11 pagesKod DeduktifMohd Fazwan MahizanPas encore d'évaluation
- Organisation and Functions of The Nervous SystemDocument110 pagesOrganisation and Functions of The Nervous SystemBoemo BolaanePas encore d'évaluation
- Drugs and Their Effects Group 6Document18 pagesDrugs and Their Effects Group 6api-252848867Pas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Zamora Memorial College 1Document13 pagesZamora Memorial College 1darylserrano07Pas encore d'évaluation
- Four Lesson Three ActivityDocument3 pagesFour Lesson Three ActivityGabriel TaylorPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)