Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Homoeopathy in Breast Cancer: AbstractsDocument5 pagesHomoeopathy in Breast Cancer: Abstractskathir_cPas encore d'évaluation
- Orthopedic PDFDocument47 pagesOrthopedic PDFSiraj HaiderPas encore d'évaluation
- On Target - Ensuring Geometric Accuracy in Radiotherapy (2008, RCR)Document76 pagesOn Target - Ensuring Geometric Accuracy in Radiotherapy (2008, RCR)Milda InayahPas encore d'évaluation
- Hirayama Disease and HomoeopathyDocument11 pagesHirayama Disease and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (3)
- De Juan, Joshua G. PE Q2 Module 6 Be Involved! Be Fit and Healthy!Document6 pagesDe Juan, Joshua G. PE Q2 Module 6 Be Involved! Be Fit and Healthy!Hanah Grace GomezPas encore d'évaluation
- Venous Disease: Chronic Venous Insufficiency Anatomical BackgroundDocument16 pagesVenous Disease: Chronic Venous Insufficiency Anatomical BackgroundSteve ColbertPas encore d'évaluation
- CIRCI Guidelines 2015Document6 pagesCIRCI Guidelines 2015Wissam SleimanPas encore d'évaluation
- 31435-Texto Do Trabalho (Obrigatório) - 135033-1-10-20230613Document7 pages31435-Texto Do Trabalho (Obrigatório) - 135033-1-10-20230613triutamisunuPas encore d'évaluation
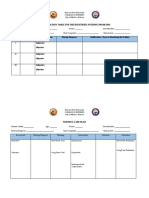
- Prioritization Table For The Identified Nursing ProblemsDocument3 pagesPrioritization Table For The Identified Nursing ProblemsMia PascualPas encore d'évaluation
- PhysiologyDocument31 pagesPhysiologyraza20100% (1)
- Planning and Managing A Dental Continuous Quality Improvement ProjectDocument35 pagesPlanning and Managing A Dental Continuous Quality Improvement ProjecttirahamdillahPas encore d'évaluation
- Rabies ReviewDocument31 pagesRabies Reviewguntur sahadiPas encore d'évaluation
- Small Renal MassDocument26 pagesSmall Renal MassSausan RasmiyyahPas encore d'évaluation
- Cholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Document47 pagesCholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Aditya SahidPas encore d'évaluation
- Public Speaking ScriptDocument2 pagesPublic Speaking Scriptsalbinarabi100% (1)
- Andres Gil Resume 2015Document3 pagesAndres Gil Resume 2015Andres GilPas encore d'évaluation
- Essential Intrapartum and Newborn CareDocument25 pagesEssential Intrapartum and Newborn CareMellePas encore d'évaluation
- Penile Inversion Vaginoplasty TechniqueDocument2 pagesPenile Inversion Vaginoplasty Techniquecathylamont816Pas encore d'évaluation
- CholesteatomaDocument29 pagesCholesteatomawhitelotusoo7Pas encore d'évaluation
- Psychotropic Drugs: Bryan Mae H. DegorioDocument65 pagesPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Asam PeroksideDocument6 pagesAsam PeroksideAsa Étudier La-DienPas encore d'évaluation
- Microbiology, Parasitology and Public Health Answer Key-RED PACOPDocument31 pagesMicrobiology, Parasitology and Public Health Answer Key-RED PACOPMelbhon Fabro Ramos100% (1)
- History Taking in Pulmonary MedicineDocument14 pagesHistory Taking in Pulmonary MedicinestudymedicPas encore d'évaluation
- Ent Mcqs 4Document7 pagesEnt Mcqs 4Uzair KhanPas encore d'évaluation
- 10 54867-jkm V9i2 123Document8 pages10 54867-jkm V9i2 123putriPas encore d'évaluation
- Section A: MCQ (80 Questions)Document16 pagesSection A: MCQ (80 Questions)Muhammed MostafaPas encore d'évaluation
- Running Head: REFLECTION ARTIFACT 1Document21 pagesRunning Head: REFLECTION ARTIFACT 1api-396212664Pas encore d'évaluation
- Internal Medicine Quiz 4 DiabetesDocument13 pagesInternal Medicine Quiz 4 DiabetesenzocruzinPas encore d'évaluation
- Presentation 5 Hand HygieneDocument26 pagesPresentation 5 Hand HygieneAfeefa Amin AliPas encore d'évaluation
- White Blood Cells (WBCS) : Total Leukocyte Count (TLC)Document7 pagesWhite Blood Cells (WBCS) : Total Leukocyte Count (TLC)Sharan MurugaboopathyPas encore d'évaluation