Vous aimerez peut-être aussi
- Hydrocarbons: David C. LeeDocument4 pagesHydrocarbons: David C. LeeSPas encore d'évaluation
- 6 HydrocarbonDocument21 pages6 HydrocarbonHeba AlhasiPas encore d'évaluation
- Toxicology Hydrocarbons: Husam Shawaqfeh Abeer MahdiDocument18 pagesToxicology Hydrocarbons: Husam Shawaqfeh Abeer MahdiHusam ShawagfehPas encore d'évaluation
- Introduction and Literature Review - 082348Document9 pagesIntroduction and Literature Review - 082348Mortada OthmanPas encore d'évaluation
- 04 FuelsDocument24 pages04 FuelsAndri Parnaungan HasibuanPas encore d'évaluation
- The Role of Gas Chromatography in Compositional Analyses in The Petroleum Industry PDFDocument16 pagesThe Role of Gas Chromatography in Compositional Analyses in The Petroleum Industry PDFPiyush SinhaPas encore d'évaluation
- Gas Travel For RRLDocument21 pagesGas Travel For RRLIrish Nicole RallosPas encore d'évaluation
- Principles of Smoking 17392Document8 pagesPrinciples of Smoking 17392Khadijah Zaimatun NisaPas encore d'évaluation
- Files Lesson Two - The Raw MaterialsDocument2 pagesFiles Lesson Two - The Raw MaterialskrulNisakPas encore d'évaluation
- Presentation On Hazop Analysis of Cumene Process: Prof. Bhakti BapatDocument26 pagesPresentation On Hazop Analysis of Cumene Process: Prof. Bhakti BapatParth0% (1)
- Cresylic Acids: Cresylic Acids Are Weak Organic Acids Which Are Partly Miscible in WaterDocument1 pageCresylic Acids: Cresylic Acids Are Weak Organic Acids Which Are Partly Miscible in WaterDinesh RajuPas encore d'évaluation
- Graphic Organizer Air PollutionDocument2 pagesGraphic Organizer Air Pollutionkwon zPas encore d'évaluation
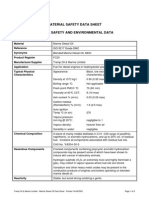
- MSDS Crude OilDocument6 pagesMSDS Crude OilFabio IkaczykPas encore d'évaluation
- Extraction of Crude Oil and Its Effect On The EnvironmentDocument9 pagesExtraction of Crude Oil and Its Effect On The EnvironmentDinesh PrabuPas encore d'évaluation
- How Refinery WorksDocument7 pagesHow Refinery WorksmuraliPas encore d'évaluation
- Module TwoDocument13 pagesModule TwoKyna PatarataPas encore d'évaluation
- Fire and Life Safety MeasuresDocument58 pagesFire and Life Safety MeasuresRhey LuceroPas encore d'évaluation
- Organic ChemistryDocument7 pagesOrganic ChemistryRoqaya BadawyPas encore d'évaluation
- Photochemical SomogDocument30 pagesPhotochemical SomogLoveleenPas encore d'évaluation
- New Coldbox BinderDocument8 pagesNew Coldbox BinderAnudatt A. Gowda100% (1)
- Marine Diesel OilDocument6 pagesMarine Diesel OilCikgu IsmaPas encore d'évaluation
- Fractional DistillationDocument6 pagesFractional Distillationagentdog175Pas encore d'évaluation
- Fuel Combustion RkrajputDocument34 pagesFuel Combustion Rkrajputsunita.storage01Pas encore d'évaluation
- Diccionario para IngenierosDocument2 pagesDiccionario para IngenieroslosmisteriosdemovillePas encore d'évaluation
- CH 2Document3 pagesCH 2MD100% (1)
- Comparision of GasketsDocument3 pagesComparision of Gasketsanwer_quadriPas encore d'évaluation
- Linde WAO TechnologyDocument30 pagesLinde WAO Technologyrzlisk01Pas encore d'évaluation
- 7.1 Carbon Compounds As Fuels and Feedstock: AlkanesDocument1 page7.1 Carbon Compounds As Fuels and Feedstock: AlkanesAmreen UnnikrishnanPas encore d'évaluation
- Ethylene & ACF PDFDocument48 pagesEthylene & ACF PDFSubrato Saha100% (2)
- Hydrocarbons UsesDocument3 pagesHydrocarbons UsesAj Benito MalidomPas encore d'évaluation
- Crude Oil - Fuels - PlasticsDocument4 pagesCrude Oil - Fuels - Plasticsagentdog175Pas encore d'évaluation
- BFP Fire Safety SeminarDocument41 pagesBFP Fire Safety SeminarAyesha Amie G. De LeonPas encore d'évaluation
- Air PollutionDocument46 pagesAir PollutionAgus PurnamaPas encore d'évaluation
- Fire Safety SeminarDocument57 pagesFire Safety SeminarErwin Marc OcampoPas encore d'évaluation
- 3.BFP BasicDocument20 pages3.BFP BasicboboyPas encore d'évaluation
- Toluene Toluene Toluene Hydrogen Chromium PlatinumDocument6 pagesToluene Toluene Toluene Hydrogen Chromium PlatinumBerry101Pas encore d'évaluation
- Hydrocarbons: SourcesDocument3 pagesHydrocarbons: Sourcesmadhangi vaithyanathanPas encore d'évaluation
- Surfactants and Their Use in Latex Technology: January 2013Document5 pagesSurfactants and Their Use in Latex Technology: January 2013herryPas encore d'évaluation
- Annual Production: BenzeneDocument12 pagesAnnual Production: BenzeneQuang Huy BùiPas encore d'évaluation
- Synthesis of Flame Retardant Dye and Its Application On Silk FabricDocument16 pagesSynthesis of Flame Retardant Dye and Its Application On Silk FabricTJPRC PublicationsPas encore d'évaluation
- Foam Breaking in Aqueous Systems: Robert J. PughDocument15 pagesFoam Breaking in Aqueous Systems: Robert J. PughMuhammad.SaimPas encore d'évaluation
- Mono Terp EnosDocument35 pagesMono Terp EnosSamantha Nascimento GomesPas encore d'évaluation
- Principles of Odorization: Edwin H. Roberson Natural Gas Odorizing, IncDocument3 pagesPrinciples of Odorization: Edwin H. Roberson Natural Gas Odorizing, IncKHALED KHALEDPas encore d'évaluation
- Mothballs 2017Document4 pagesMothballs 2017Akshay BaidPas encore d'évaluation
- Chemistry Notes (Organic Chem)Document6 pagesChemistry Notes (Organic Chem)Teo Jia Ming NickolasPas encore d'évaluation
- Comparison of Equilibrium-Stage and Rate-Based ModDocument23 pagesComparison of Equilibrium-Stage and Rate-Based ModValeria CarrilloPas encore d'évaluation
- Petroleum Refinery Engineering PP-414: Dr. Saud HashmiDocument29 pagesPetroleum Refinery Engineering PP-414: Dr. Saud Hashmiayesha naseerPas encore d'évaluation
- 4th Quarter Applied Chemistry 1Document10 pages4th Quarter Applied Chemistry 1Jasmine Anne LapizarPas encore d'évaluation
- Waste Lubricating-1Document4 pagesWaste Lubricating-1Tiffany noor afifPas encore d'évaluation
- Soot Formation: Institut Ffir Physikalische Chemic Der Universiti T Gi Ttinoen, 3400 Gbttingen, West German)Document45 pagesSoot Formation: Institut Ffir Physikalische Chemic Der Universiti T Gi Ttinoen, 3400 Gbttingen, West German)MahmoudKamalElshazlyPas encore d'évaluation
- Catalytic Naphtha Reforming: January 2006Document12 pagesCatalytic Naphtha Reforming: January 2006AsifPas encore d'évaluation
- Industrial ExplosivesDocument2 pagesIndustrial ExplosivesAlliah Mae LumanogPas encore d'évaluation
- AkzoNobel MEA PIS Tcm53-24552Document1 pageAkzoNobel MEA PIS Tcm53-24552Desi Apriyanti RahayuPas encore d'évaluation
- Untitled PresentationDocument5 pagesUntitled Presentationasad blablaPas encore d'évaluation
- Polymers: Green Enhanced Oil Recovery For Carbonate ReservoirsDocument31 pagesPolymers: Green Enhanced Oil Recovery For Carbonate Reservoirskyaw nyiPas encore d'évaluation
- Preparation, Characterization, and Evaluation of Some Ashless Detergent-Dispersant Additives For Lubricating Engine OilDocument10 pagesPreparation, Characterization, and Evaluation of Some Ashless Detergent-Dispersant Additives For Lubricating Engine OilNelson Enrique Bessone MadridPas encore d'évaluation
- Industrial ExplosivesDocument9 pagesIndustrial ExplosivesAmlan MajumdarPas encore d'évaluation
- Gen ChemDocument3 pagesGen ChemCharles LowiePas encore d'évaluation
- Polymer Syntheses: Organic Chemistry: A Series of Monographs, Vol. 3D'EverandPolymer Syntheses: Organic Chemistry: A Series of Monographs, Vol. 3Pas encore d'évaluation
- Principle of Digestion, Digestive Juices - Composition, Phases of Secretion, Regulations and FunctionsDocument31 pagesPrinciple of Digestion, Digestive Juices - Composition, Phases of Secretion, Regulations and FunctionsRaju NiraulaPas encore d'évaluation
- 3.list of AbbreviationsDocument3 pages3.list of AbbreviationsRaju NiraulaPas encore d'évaluation
- Biomarkers in DiabetisDocument24 pagesBiomarkers in DiabetisRaju NiraulaPas encore d'évaluation
- Antineoplastic S NotesDocument8 pagesAntineoplastic S NotesRaju NiraulaPas encore d'évaluation
- Pharmacist Register at Ion ProcedureDocument25 pagesPharmacist Register at Ion ProcedureAhmad Faheem Qureshi100% (1)
- PRESENTED:-Dr. Raju NiraulaDocument29 pagesPRESENTED:-Dr. Raju NiraulaRaju NiraulaPas encore d'évaluation
- Preparation of Penicillins by Acylation of 6-Aminopenicillanic Acid With Acyl Chlorides Week One: SynthesisDocument6 pagesPreparation of Penicillins by Acylation of 6-Aminopenicillanic Acid With Acyl Chlorides Week One: SynthesisRaju NiraulaPas encore d'évaluation
- Analgesics Best PDFDocument57 pagesAnalgesics Best PDFRaju NiraulaPas encore d'évaluation
- Expert PTE B2 AnswerDocument100 pagesExpert PTE B2 AnswerAbo Moussa75% (8)
- A Modified Method For The Synthesiss of Nitrofurazone: January 2003Document4 pagesA Modified Method For The Synthesiss of Nitrofurazone: January 2003Raju NiraulaPas encore d'évaluation
- Antiprotozoaldrugatheirmodeofaction 170318180554Document36 pagesAntiprotozoaldrugatheirmodeofaction 170318180554Raju NiraulaPas encore d'évaluation
- Antihistamines: Student Learning GoalsDocument45 pagesAntihistamines: Student Learning GoalsDaniel WangPas encore d'évaluation
- PTE Essays With AnswersDocument15 pagesPTE Essays With Answersnarasimha93% (307)
- Preparation of Penicillins by Acylation of 6-Aminopenicillanic Acid With Acyl Chlorides Week One: SynthesisDocument6 pagesPreparation of Penicillins by Acylation of 6-Aminopenicillanic Acid With Acyl Chlorides Week One: SynthesisRaju NiraulaPas encore d'évaluation
- Anti Ulcerdrugs 150515191630 Lva1 App6891Document33 pagesAnti Ulcerdrugs 150515191630 Lva1 App6891Raju NiraulaPas encore d'évaluation
- 1482225085Document156 pages1482225085tediPas encore d'évaluation
- Dickson, Charles - Experiments in Pharmaceutical Chemistry-CRC Press (2014)Document67 pagesDickson, Charles - Experiments in Pharmaceutical Chemistry-CRC Press (2014)Raju NiraulaPas encore d'évaluation
- Anti Ulcerdrugs 150515191630 Lva1 App6891Document33 pagesAnti Ulcerdrugs 150515191630 Lva1 App6891Raju NiraulaPas encore d'évaluation
- Antiparkinsonics (Parkinson Has No Cure As of 2014 Drugs Only Control Symptoms)Document31 pagesAntiparkinsonics (Parkinson Has No Cure As of 2014 Drugs Only Control Symptoms)Raju NiraulaPas encore d'évaluation
- Clinical Pharmacy: Sohan Patel Assistant Professor, Modasa, Gujarat, IndiaDocument56 pagesClinical Pharmacy: Sohan Patel Assistant Professor, Modasa, Gujarat, IndiaRaju NiraulaPas encore d'évaluation
- 2nd YearDocument33 pages2nd YearRaju NiraulaPas encore d'évaluation
- Antiparkinsonics (Parkinson Has No Cure As of 2014 Drugs Only Control Symptoms)Document31 pagesAntiparkinsonics (Parkinson Has No Cure As of 2014 Drugs Only Control Symptoms)Raju NiraulaPas encore d'évaluation
- PracticalsDocument16 pagesPracticalsRaju NiraulaPas encore d'évaluation
- Dr. Patrick J. Bryant Pharm.D. FSCIP, Dr. Heather A. Pace Pharm.D. - The Pharmacist's Guide To Evidence-Based Medicine For Clinical Decision Making-ASHP (2008) PDFDocument209 pagesDr. Patrick J. Bryant Pharm.D. FSCIP, Dr. Heather A. Pace Pharm.D. - The Pharmacist's Guide To Evidence-Based Medicine For Clinical Decision Making-ASHP (2008) PDFRaju Niraula100% (1)
- Opiod AnalgesicsDocument66 pagesOpiod AnalgesicsRaju NiraulaPas encore d'évaluation
- Binder PDFDocument55 pagesBinder PDFRaju NiraulaPas encore d'évaluation
- CSMT To MaoDocument3 pagesCSMT To Maoraju niraulaPas encore d'évaluation
- SCRIPTS - Cambridge Ielts 1Document43 pagesSCRIPTS - Cambridge Ielts 1Raju NiraulaPas encore d'évaluation
- Principle of Organic Medicine ChemistryDocument331 pagesPrinciple of Organic Medicine ChemistryVamgipuram Shashank100% (1)
- 4: Stereochemistry: PreviewDocument51 pages4: Stereochemistry: PreviewRaju NiraulaPas encore d'évaluation
- Computer System Servicing 1 NC-II MODULE 8A (Second Semester: Week 6 - 7)Document19 pagesComputer System Servicing 1 NC-II MODULE 8A (Second Semester: Week 6 - 7)Carl John GomezPas encore d'évaluation
- Essentials: Week by WeekDocument18 pagesEssentials: Week by WeekHirenkumar ShahPas encore d'évaluation
- 160kW SOFT STARTER - TAP HOLE 1Document20 pages160kW SOFT STARTER - TAP HOLE 1Ankit Uttam0% (1)
- Adaptive Leadership: Leadership: Theory and PracticeDocument14 pagesAdaptive Leadership: Leadership: Theory and PracticeJose Daniel Quintero100% (1)
- A2Document4 pagesA2Akshay KumarPas encore d'évaluation
- Chapter 2.3.3 History of Visual Arts Modernism Post ModernismDocument17 pagesChapter 2.3.3 History of Visual Arts Modernism Post ModernismKim Ashley SarmientoPas encore d'évaluation
- Liquitex Soft Body BookletDocument12 pagesLiquitex Soft Body Booklethello belloPas encore d'évaluation
- Riqas Ri RQ9142 11aDocument6 pagesRiqas Ri RQ9142 11aGrescia Ramos VegaPas encore d'évaluation
- Classification of Books Using Python and FlaskDocument5 pagesClassification of Books Using Python and FlaskIJRASETPublicationsPas encore d'évaluation
- Bench-Scale Decomposition of Aluminum Chloride Hexahydrate To Produce Poly (Aluminum Chloride)Document5 pagesBench-Scale Decomposition of Aluminum Chloride Hexahydrate To Produce Poly (Aluminum Chloride)varadjoshi41Pas encore d'évaluation
- Body Systems Portfolio - Tommy JDocument8 pagesBody Systems Portfolio - Tommy Japi-554072790Pas encore d'évaluation
- 35 Electrical Safety SamanDocument32 pages35 Electrical Safety SamanSaman Sri Ananda RajapaksaPas encore d'évaluation
- Java Complete Collection FrameworkDocument28 pagesJava Complete Collection FrameworkkhushivanshPas encore d'évaluation
- UAV Design TrainingDocument17 pagesUAV Design TrainingPritam AshutoshPas encore d'évaluation
- Concrete Specification (BS8500)Document3 pagesConcrete Specification (BS8500)teh100% (1)
- Reaction Paper FinalDocument5 pagesReaction Paper FinalJelo RoxasPas encore d'évaluation
- GCP Vol 2 PDF (2022 Edition)Document548 pagesGCP Vol 2 PDF (2022 Edition)Sergio AlvaradoPas encore d'évaluation
- Academic Socialization and Its Effects On Academic SuccessDocument2 pagesAcademic Socialization and Its Effects On Academic SuccessJustin LargoPas encore d'évaluation
- Motivation Theories Description and CriticismDocument14 pagesMotivation Theories Description and CriticismAhmed Elgazzar89% (18)
- Procter and Gamble - MarketingDocument10 pagesProcter and Gamble - MarketingIvana Panovska100% (5)
- Arbans Complete Conservatory Method For Trumpet Arbans Complete ConservatoryDocument33 pagesArbans Complete Conservatory Method For Trumpet Arbans Complete ConservatoryRicardo SoldadoPas encore d'évaluation
- Stonehell Dungeon 1 Down Night Haunted Halls (LL)Document138 pagesStonehell Dungeon 1 Down Night Haunted Halls (LL)some dude100% (9)
- ETNOBotanica NombresDocument188 pagesETNOBotanica Nombresjalepa_esPas encore d'évaluation
- BSH 7005-15Document129 pagesBSH 7005-15Mark InnesPas encore d'évaluation
- 4B - Urp - Shavya's FarmDocument22 pages4B - Urp - Shavya's FarmSnehansh KishorePas encore d'évaluation
- Honda IzyDocument16 pagesHonda IzyTerry FordPas encore d'évaluation
- MDI - Good Fellas - ScriptDocument20 pagesMDI - Good Fellas - ScriptRahulSamaddarPas encore d'évaluation
- IOT Questions and Answers - SolutionDocument8 pagesIOT Questions and Answers - SolutionOmar CheikhrouhouPas encore d'évaluation
- Changed Report 2015 PDFDocument298 pagesChanged Report 2015 PDFAnonymous FKjeRG6AFnPas encore d'évaluation
- Enrile v. SalazarDocument26 pagesEnrile v. SalazarMaria Aerial AbawagPas encore d'évaluation