Vous aimerez peut-être aussi
- Leave Application Form UCPTDocument1 pageLeave Application Form UCPTMarlon AbellanaPas encore d'évaluation
- The Islamia University of Bahawalpur Rahim Yar Khan Campus: Serial No . Leave ApplicationDocument2 pagesThe Islamia University of Bahawalpur Rahim Yar Khan Campus: Serial No . Leave ApplicationSafoora SiddiquaPas encore d'évaluation
- Leave FormDocument1 pageLeave FormEdmore MukotsanjeraPas encore d'évaluation
- Sliver Water Bangladesh Limited: Leave AllowedDocument1 pageSliver Water Bangladesh Limited: Leave AllowedTMPas encore d'évaluation
- International Islamic University Malaysia Eye Specialist ClinicDocument1 pageInternational Islamic University Malaysia Eye Specialist ClinicAminul HakimPas encore d'évaluation
- DTR Sample - Excel SubmissionDocument10 pagesDTR Sample - Excel SubmissionJulina AredidonPas encore d'évaluation
- FSQ14 Leave Application (03 August 2022) Rev 3.0Document1 pageFSQ14 Leave Application (03 August 2022) Rev 3.0Rejo AbrahamPas encore d'évaluation
- Mac & Rains Pharmaceutical (PVT.) LTD.: Leave Application FormDocument1 pageMac & Rains Pharmaceutical (PVT.) LTD.: Leave Application Formusman javaidPas encore d'évaluation
- Absence Form 2Document1 pageAbsence Form 2Mihaela NicoarăPas encore d'évaluation
- Leave Request FormDocument1 pageLeave Request Formjoseph swaidPas encore d'évaluation
- 011 Leave Application FormDocument1 page011 Leave Application FormSolehah OthmanPas encore d'évaluation
- Certification of LeaveDocument1 pageCertification of LeaveMolly SchneidPas encore d'évaluation
- Leave RequestDocument2 pagesLeave RequestDinuPas encore d'évaluation
- Acknowledgement ReceiptDocument17 pagesAcknowledgement ReceiptEula Chua YlaganPas encore d'évaluation
- Leave Request FormDocument1 pageLeave Request Formmikeronoh148Pas encore d'évaluation
- Lve Format 100Document2 pagesLve Format 100satyapennintiPas encore d'évaluation
- Leave Request Form: RemarkDocument1 pageLeave Request Form: RemarkMichael JordanPas encore d'évaluation
- Clearance FormDocument3 pagesClearance FormMuhammad Rashed NadeemPas encore d'évaluation
- HRD Form 004 - Request For Leave of AbsenceDocument1 pageHRD Form 004 - Request For Leave of AbsenceWynn DizonPas encore d'évaluation
- Reimbursement Expense Receipt Reimbursement Expense ReceiptDocument1 pageReimbursement Expense Receipt Reimbursement Expense ReceiptMark Calpon Lechido100% (1)
- DTR Sample - Excel SubmissionDocument8 pagesDTR Sample - Excel SubmissionJulina AredidonPas encore d'évaluation
- Request For LeaveDocument1 pageRequest For LeaveJanine O'shea DoloresPas encore d'évaluation
- I Owe You Debt Acknowledgment FormDocument1 pageI Owe You Debt Acknowledgment FormEvelyn Vizconde100% (1)
- HSC - Leave FormDocument1 pageHSC - Leave Formbanneytkw1004Pas encore d'évaluation
- Client Request FormDocument1 pageClient Request FormDenald Paz100% (1)
- CSC Form 6Document1 pageCSC Form 6Eurika Lage NiPas encore d'évaluation
- 10-Leave Application Form StaffDocument1 page10-Leave Application Form Staffsheenaparveen31Pas encore d'évaluation
- 2023-0112-Endorsement Form 2Document1 page2023-0112-Endorsement Form 2Franco SenaPas encore d'évaluation
- FNF Clearance FormDocument3 pagesFNF Clearance Formaparna kPas encore d'évaluation
- PFL New Form 4 1Document3 pagesPFL New Form 4 1Neil PilosopoPas encore d'évaluation
- Application For LeaveDocument1 pageApplication For Leavevinmar28Pas encore d'évaluation
- Leave of Absence Form (Rev. 02 072017)Document1 pageLeave of Absence Form (Rev. 02 072017)KIMBERLY BALISACANPas encore d'évaluation
- Leave Application FormDocument1 pageLeave Application FormMuhammad ArifPas encore d'évaluation
- SSSForm ADA EnrollmentDocument2 pagesSSSForm ADA EnrollmentJohnbree BreePas encore d'évaluation
- Leave Request FormDocument1 pageLeave Request Formmuneeb.engineer10Pas encore d'évaluation
- Ayda Realty & Dev't. Corp. Change of Schedule: Change Shift Change Rest Day From TO From TODocument2 pagesAyda Realty & Dev't. Corp. Change of Schedule: Change Shift Change Rest Day From TO From TOAydarealty CorpPas encore d'évaluation
- Joint Loan DeclarationDocument2 pagesJoint Loan Declarationp hem prasadPas encore d'évaluation
- BOSA Loan FormDocument2 pagesBOSA Loan FormIsaac OkotPas encore d'évaluation
- Leave Application FormDocument2 pagesLeave Application FormPurchase DeptPas encore d'évaluation
- Leave Request FormDocument1 pageLeave Request FormEdhilyn HurryPas encore d'évaluation
- Leave Application FormDocument1 pageLeave Application Formwentao0420Pas encore d'évaluation
- Application For Leave of Absence: (To Be Submitted Before Actually Taking Leave)Document5 pagesApplication For Leave of Absence: (To Be Submitted Before Actually Taking Leave)Maricor MontemorPas encore d'évaluation
- Leave Appli Form 2Document1 pageLeave Appli Form 2Manette FernandezPas encore d'évaluation
- AG&P - Application Form - 01 Oct 2017Document2 pagesAG&P - Application Form - 01 Oct 2017Justine Matthan DimaculanganPas encore d'évaluation
- SENA FORM No. 5 - Quitclaim and ReleaseDocument1 pageSENA FORM No. 5 - Quitclaim and Releasepierremartinreyes100% (1)
- Ob FormDocument1 pageOb FormRpee Julie De GuzmanPas encore d'évaluation
- Leave Application Form SampleDocument1 pageLeave Application Form SamplePrantik28Pas encore d'évaluation
- Reimbursement Expense Receipt Reimbursement Expense ReceiptDocument1 pageReimbursement Expense Receipt Reimbursement Expense ReceiptJUN REY GUBATONPas encore d'évaluation
- Petty Cash Voucher: Appendix 33Document2 pagesPetty Cash Voucher: Appendix 33hehehedontmind mePas encore d'évaluation
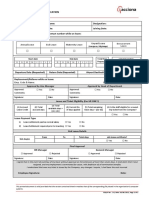
- Employee Details Name of Employee: Employee Code Number: Department: Designation: Relocation Date of JoiningDocument2 pagesEmployee Details Name of Employee: Employee Code Number: Department: Designation: Relocation Date of JoiningKumarRavi RanjanPas encore d'évaluation
- Leave Application Form: Use Electronics (M) Sdn. Bhd. (314642-W)Document1 pageLeave Application Form: Use Electronics (M) Sdn. Bhd. (314642-W)ijam CoreMadridPas encore d'évaluation
- Leave Notification Leave Notification: Admin/201 Admin/201Document7 pagesLeave Notification Leave Notification: Admin/201 Admin/201ilaw atbpPas encore d'évaluation
- Provident Loan FormDocument3 pagesProvident Loan FormrobotmatinoPas encore d'évaluation
- Leave Application FormDocument1 pageLeave Application Formarshed777Pas encore d'évaluation
- Disbursement Voucher: A Certified: B Certified: C CertifiedDocument1 pageDisbursement Voucher: A Certified: B Certified: C CertifiedEidorian PajPas encore d'évaluation
- Permit To Leave Premises Permit To Leave PremisesDocument3 pagesPermit To Leave Premises Permit To Leave PremisesjohnmarcPas encore d'évaluation
- Form Cuti 2022 LDocument3 pagesForm Cuti 2022 LelchandraPas encore d'évaluation
- Appendix 48 - PCVDocument1 pageAppendix 48 - PCVwichupinunoPas encore d'évaluation
- Leave Form (Blank)Document1 pageLeave Form (Blank)Moshe Jamero GamosPas encore d'évaluation
- Request LetterDocument1 pageRequest LetterPrincessAntonetteDeCastro100% (1)
- Letter of IntentDocument1 pageLetter of IntentPrincessAntonetteDeCastroPas encore d'évaluation
- Philippine National Bank (PNB) Princess Antonette de Castro 5240466560287122Document1 pagePhilippine National Bank (PNB) Princess Antonette de Castro 5240466560287122PrincessAntonetteDeCastroPas encore d'évaluation
- Integrated Management System PolicyDocument2 pagesIntegrated Management System PolicyPrincessAntonetteDeCastroPas encore d'évaluation
- Company ProfileDocument8 pagesCompany ProfilePrincessAntonetteDeCastroPas encore d'évaluation
- ClearanceDocument1 pageClearancePrincessAntonetteDeCastroPas encore d'évaluation
- RAVAGO Mission StatementDocument1 pageRAVAGO Mission StatementPrincessAntonetteDeCastroPas encore d'évaluation
- 13 Month PayDocument56 pages13 Month PayPrincessAntonetteDeCastroPas encore d'évaluation
- Lord We Gather Today PDFDocument3 pagesLord We Gather Today PDFPrincessAntonetteDeCastro100% (4)
- Company IdDocument2 pagesCompany IdPrincessAntonetteDeCastroPas encore d'évaluation
- Sack Sentence Completion Test and Answer SheetDocument1 pageSack Sentence Completion Test and Answer SheetPrincessAntonetteDeCastro100% (1)
- Ate BelDocument2 pagesAte BelPrincessAntonetteDeCastroPas encore d'évaluation
- Manila WEST 2: Sunday, May 15, 2016Document10 pagesManila WEST 2: Sunday, May 15, 2016PrincessAntonetteDeCastroPas encore d'évaluation
- SenaDocument21 pagesSenaPrincessAntonetteDeCastroPas encore d'évaluation
- October 12, 2016: Area HR of Manila West 1Document1 pageOctober 12, 2016: Area HR of Manila West 1PrincessAntonetteDeCastroPas encore d'évaluation
- Ravago Equipment Rentals, Inc.: Organizational ChartDocument7 pagesRavago Equipment Rentals, Inc.: Organizational ChartPrincessAntonetteDeCastroPas encore d'évaluation
- Himig Pasko George Hernandez PDFDocument16 pagesHimig Pasko George Hernandez PDFAnselmoCapuliPas encore d'évaluation
- Loving Christ in The Needy and The Forsaken: National Seafarers' Day / Start of Laity WeekDocument4 pagesLoving Christ in The Needy and The Forsaken: National Seafarers' Day / Start of Laity WeekPrincessAntonetteDeCastroPas encore d'évaluation
- Shop Boni Shop Makati Shop Finance Monumento Cainta ShopDocument11 pagesShop Boni Shop Makati Shop Finance Monumento Cainta ShopPrincessAntonetteDeCastroPas encore d'évaluation
- Alexnader Borres AbsentDocument1 pageAlexnader Borres AbsentPrincessAntonetteDeCastroPas encore d'évaluation
- Drug Free Policy RomaiDocument4 pagesDrug Free Policy RomaiPrincessAntonetteDeCastroPas encore d'évaluation
- Nuestro Señor de Longos ChoirDocument7 pagesNuestro Señor de Longos ChoirPrincessAntonetteDeCastroPas encore d'évaluation
- Ash Wednesday EuchaletteDocument4 pagesAsh Wednesday EuchalettePrincessAntonetteDeCastro0% (1)
- Reinforcement 2nd Term IIDocument3 pagesReinforcement 2nd Term IICorinaBalanPas encore d'évaluation
- PMR Writing TipsDocument6 pagesPMR Writing TipsNadiah Bt Mohd AbdahPas encore d'évaluation
- Present Simple: B) FinishesDocument4 pagesPresent Simple: B) Finishesjuan camilo madariaga mangonesPas encore d'évaluation
- LA Metro - 169Document2 pagesLA Metro - 169cartographica100% (1)
- Word Formation Travel Arrangements 1Document3 pagesWord Formation Travel Arrangements 1Sentido Común Alternativo SCAPas encore d'évaluation
- Holiday ListDocument1 pageHoliday Listankitaagarwal89Pas encore d'évaluation
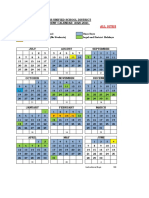
- Travis Unified School District STUDENT CALENDAR 2020-2021: All SitesDocument1 pageTravis Unified School District STUDENT CALENDAR 2020-2021: All Sitesapi-290711805Pas encore d'évaluation
- Holiday/Vacation Policy: Annual HolidaysDocument18 pagesHoliday/Vacation Policy: Annual HolidaysmalaysianheartPas encore d'évaluation
- Task 6 - Final ExamDocument11 pagesTask 6 - Final ExamMaría Camila GómezPas encore d'évaluation
- Pumpkin: The Curious History of An American IconDocument12 pagesPumpkin: The Curious History of An American IconUniversity of Washington Press50% (2)
- Key - Practice Test No. 1 - TET HOLIDAYDocument2 pagesKey - Practice Test No. 1 - TET HOLIDAYKiều Bảo NgânPas encore d'évaluation
- Tugas Uas Miss LennyDocument8 pagesTugas Uas Miss LennyZiyan Khoirun hakimPas encore d'évaluation
- Unit 7 . On Vacation! (3re. Percial)Document4 pagesUnit 7 . On Vacation! (3re. Percial)Brahian PerezPas encore d'évaluation
- School Calendar 2019 2020 HomeschoolDocument2 pagesSchool Calendar 2019 2020 HomeschoolJoyce Ann SameraPas encore d'évaluation
- Paoli / Thorndale Line: Saturdays Sundays and Major HolidaysDocument5 pagesPaoli / Thorndale Line: Saturdays Sundays and Major HolidaysTu Le ThanhPas encore d'évaluation
- 2012 ZNO EnglishDocument16 pages2012 ZNO EnglishJulia DankovychPas encore d'évaluation
- Bruno Is From Italy He Went On Holidays With His Father Last WinterDocument1 pageBruno Is From Italy He Went On Holidays With His Father Last WinterJuan Carlos LugoPas encore d'évaluation
- Banyan Tree Case Study 18BM61K24Document2 pagesBanyan Tree Case Study 18BM61K24Arup Kumar Pyne100% (1)
- LIRRDocument2 pagesLIRRMinina AjmeraPas encore d'évaluation
- The Maharashtra Employees of Private Schools Act.Document72 pagesThe Maharashtra Employees of Private Schools Act.Harshvardhan BorsePas encore d'évaluation
- Lawsuit Against Measure TDocument12 pagesLawsuit Against Measure TBen MargiottPas encore d'évaluation
- The Ultimate Festivities PackDocument210 pagesThe Ultimate Festivities PackJasmina Cickarik100% (2)
- Adventure Series Catalog-Opt PDFDocument24 pagesAdventure Series Catalog-Opt PDFDeux ArtsPas encore d'évaluation
- Rossette Grand Vacation - Google Search PDFDocument1 pageRossette Grand Vacation - Google Search PDFShahroz KhanPas encore d'évaluation
- Best Tourist Spots in The PhilippinesDocument3 pagesBest Tourist Spots in The PhilippinesJustine Ian Cellona GalgoPas encore d'évaluation
- TripAdvisor: Read Reviews, Compare Prices & BookDocument4 pagesTripAdvisor: Read Reviews, Compare Prices & BooknorthstarleoPas encore d'évaluation
- Helping Children Be The Best They Can Be Dear Parents, Governors and ChildrenDocument4 pagesHelping Children Be The Best They Can Be Dear Parents, Governors and ChildrencentralwebadminPas encore d'évaluation
- Exercícios Extras de InglêsDocument2 pagesExercícios Extras de InglêsAna Luiza Valentim100% (1)
- Blas OpleDocument1 pageBlas OpleJedd SantosPas encore d'évaluation
- De 24Document4 pagesDe 24longle1604Pas encore d'évaluation