Académique Documents
Professionnel Documents
Culture Documents
Semiinvasive Pulmonary Aspergillosis in Chronic Obstructive Pulmonary Disease
Transféré par
ekaTitre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Semiinvasive Pulmonary Aspergillosis in Chronic Obstructive Pulmonary Disease
Transféré par
ekaDroits d'auteur :
Formats disponibles
Semiinvasive Pulmonary
Aspergillosis in Chronic
Downloaded from www.ajronline.org by 36.78.24.119 on 11/05/14 from IP address 36.78.24.119. Copyright ARRS. For personal use only; all rights reserved
Obstructive Pulmonary Disease:
Radiologic and Pathologic Findings in
Nine Patients
Toms Franquet 1 OBJECTIVE. The purpose of this study is to assess the radiographic, thin-section CT, and
Nestor L. Mller 2 histologic findings of semiinvasive aspergillosis in patients with chronic obstructive pulmo-
Ana Gimnez 1 nary disease (COPD).
Pere Domingo 3 MATERIALS AND METHODS. The study included nine patients with COPD seen at
the Hospital de Sant Pau during a 3-year period who had histopathologically proven as-
Vicente Plaza 3
pergillosis with tissue invasion. Chest radiography and thin-section (2-mm collimation) CT of
Ramn Bordes 4
the chest were available in all cases.
RESULTS. Nine patients had semiinvasive aspergillosis proven at autopsy (n = 7) or by thora-
coscopically guided lung biopsy (n = 2). The radiologic findings consisted of parenchymal con-
solidation (n = 6) and nodules larger than 1 cm in diameter (n = 3). Parenchymal consolidation
involved the upper lobes in five patients and was bilateral in four. Cavitation was present in two of
the patients with consolidation and in two of the patients with nodular opacities. Adjacent pleural
thickening was revealed by CT in four patients. Histologically, the areas of consolidation repre-
sented active inflammation and intraalveolar hemorrhage containing Aspergillus organisms. In
the three patients with multiple cavitated nodules, a variable degree of central necrosis was ob-
served. The inflammatory infiltrate extended into the surrounding lung parenchyma, and adjacent
areas of hemorrhage were also seen. Aspergillus colonies were identified within the lung tissue.
CONCLUSION. Upper lobe consolidation or multiple nodules in patients with COPD
should raise the possibility of semiinvasive aspergillosis.
M
ost pulmonary diseases caused by pleural thickening, and may be indistinguishable
Aspergillus have been categorized from pulmonary tuberculosis [3, 4].
as invasive, saprophytic, or allergic Limited information is available about the
[1, 2]. However, semiinvasive aspergillosis, also CT findings and the histologic basis for the ra-
called chronic necrotizing aspergillosis, has re- diologic abnormalities. Respiratory infection
cently been recognized as a different type of in- is an important cause of morbidity and mortal-
Received April 7, 1999; accepted after revision fection that does not fit into the three traditional ity in patients with COPD. Accurate diagnostic
June 21, 1999.
1
categories [3, 4]. Although invasive forms of as- evaluation and familiarity with the radiologic
Department of Radiology, Hospital de Sant Pau,
Universidad Autnoma de Barcelona, San Antonio M.
pergillosis involve previously healthy areas of manifestations of semiinvasive aspergillosis is
Claret 167, 08025, Barcelona, Spain. Address lung as a complication of an immunosup- necessary to guide proper therapy and improve
correspondence to T. Franquet. pressed state [5, 6], semiinvasive aspergillosis is patient survival [10].
2
Department of Radiology, University of British Columbia more indolent and tends to occur in patients The purpose of the present study was to eval-
and Vancouver Hospital and Health Sciences Centre, who have mildly impaired immunity due to uate the radiographic and thin-section CT find-
855 W. 12th Ave., Vancouver, British Columbia, V5Z 1M9
Canada. chronic debilitating illness, advanced age, or ings of semiinvasive pulmonary aspergillosis
3
Department of Internal Medicine, Hospital de Sant Pau,
prolonged corticosteroid administration, or in infection in patients with COPD and to compare
Universidad Autnoma de Barcelona, 08025, Barcelona, patients with underlying bronchiectasis or the radiologic with the histologic findings.
Spain. chronic obstructive pulmonary disease (COPD)
4
Department of Pathology, Hospital de Sant Pau, [3, 4, 79]. Some studies suggest that semiinva- Materials and Methods
Universidad Autnoma de Barcelona, 08025, Barcelona, sive aspergillosis is increasing in frequency and Patients
Spain.
may be severe or fatal if untreated [8, 9]. From January 1995 through July 1998, all pa-
AJR 2000;174:5156
The radiographic appearance of semiinvasive tients with COPD and pathologic evidence of semi-
0361-803X/00/174151 pulmonary aspergillosis has been described as invasive pulmonary aspergillosis were identified by
American Roentgen Ray Society consisting mainly of upper lobe consolidation and a review of the pathology database records in the
AJR:174, January 2000 51
Franquet et al.
department of pathology at the Hospital de Sant Pau. time of 2 sec. All images were obtained at window Results
The records of nine smokers with COPD and a levels appropriate for lung parenchyma (window Most patients (n = 7) had COPD of the
pathologically proven diagnosis of semiinvasive as- width, 1700 H; window level, 600 H) and mediasti- chronic bronchitis type, whereas two had centri-
pergillosis were reviewed. Semiinvasive aspergillo- num (window width, 350 H; window level, 50 H). lobular emphysema affecting predominantly
sis was diagnosed at autopsy in seven patients and
the upper lobes. Five patients had received
by thoracoscopically guided biopsy in two patients. Review of the Images
Chest radiographs and CT scans were indepen-
low-dose corticosteroid treatment for COPD.
All patients had undergone both conventional chest
Six patients had received antibiotics for sus-
Downloaded from www.ajronline.org by 36.78.24.119 on 11/05/14 from IP address 36.78.24.119. Copyright ARRS. For personal use only; all rights reserved
radiography and CT. The patients were all men with dently evaluated by two chest radiologists, and the
a mean age of 68 years (range, 5489 years). interpretation was reached by consensus only when pected pulmonary infection that was not respon-
discrepancies were identified. The conventional sive to therapy. Three patients were alcoholics,
Imaging Technique chest radiographs and the corresponding CT images one had diabetes, and one had chronic renal in-
All CT examinations were performed with a were reviewed. Conventional chest radiographs and sufficiency. Symptoms and signs at presentation
Toshiba 900 CT unit (Toshiba Medical Systems, To- CT scans were analyzed for the presence of paren- included cough (eight patients, 89%), sputum
kyo, Japan). Thin-collimation (2-mm) sections were chymal consolidation, cavitation, nodules, pleural (seven patients, 78%), fever (six patients, 67%),
obtained at 10-mm intervals extending from the lung thickening or fluid, bronchiectasis, and any other shortness of breath (five patients, 56%), and he-
apices to below the costophrenic angles. A 35-cm significant finding. The distribution of lesions was
moptysis (two patients, 22%). Histologic and
field of view and a 512 512 reconstruction matrix recorded as predominantly in the upper, middle, or
were used. Images were reconstructed with a lower lung zone, and as predominantly central, pe-
microbiologic proof of semiinvasive aspergillo-
high-spatial-frequency algorithm for parenchymal ripheral, or random. sis was obtained from specimens taken at au-
analysis and with a standard algorithm for mediasti- Histopathologic diagnosis was based on histo- topsy (n = 7) or at thoracoscopically guided
nal evaluation. CT scans were obtained at the sus- logic findings of Aspergillus colonies in the bron- biopsy (n = 2). Before death, all the patients had
pended end-inspiratory volume with an imaging chial tree and lung parenchyma. received a diagnosis of probable semiinvasive
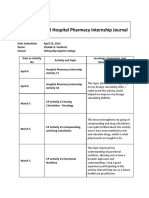
Fig. 1.Semiinvasive pulmonary
A B aspergillosis in 72-year-old man
with centrilobular emphysema and
2-month history of cough and chest
discomfort at presentation.
A, Posteroanterior chest radiograph
shows peripheral and right apical
air-space consolidation.
B, CT scan obtained at same level as A
shows segmental air-space consolida-
tion in posterior segment of right upper
lobe that contains multiple low-attenu-
ation areas (arrowheads), small air
bubbles, and punctate calcifications.
C, Photomicrograph of biopsy speci-
men obtained from right upper lobe
reveals widespread intraalveolar exu-
dative eosinophil material mixed with
acute inflammatory cells, macro-
phages, and fungal hyphae (straight
arrows). Microabscess containing As-
pergillus fumigatus colonies (curved
arrows) corresponds to low-attenua-
tion areas seen on B. (H and E, 400)
C
52 AJR:174, January 2000
Semiinvasive Pulmonary Aspergillosis
aspergillosis based on clinical, microbiologic, was located predominantly or exclusively in three patients; multiple cavities were identi-
and radiologic criteria [3, 7]. the upper lobes in five patients. Areas of cav- fied in two patients. Other findings included
On conventional chest radiographs, areas itation were present in two patients. Multiple pleural thickening in four patients and myce-
of consolidation were identified in six pa- pulmonary nodules measuring greater than 1 tomas seen on radiography in one patient.
tients; the areas were multiple and bilateral cm in diameter without associated halos of On CT, the areas of consolidation were
in four and focal in two. The consolidation ground-glass attenuation were present in shown to be segmental in all six patients. Ad-
jacent pleural thickening was identified on
Downloaded from www.ajronline.org by 36.78.24.119 on 11/05/14 from IP address 36.78.24.119. Copyright ARRS. For personal use only; all rights reserved
CT in four patients (Fig. 1). Cavities seen in
two patients with consolidation had irregular
walls and ranged in size from 1 to 4 cm (Fig.
2). The multiple nodular opacities present on
CT in three patients had ill-defined margins.
Multiple cavitations were seen in two patients
with nodules. Mycetomas were identified on
CT in two patients (Fig. 3).
Histologic examination in the six patients
with parenchymal consolidation on radiogra-
phy and CT showed Aspergillus organisms in
alveolar spaces, intraalveolar hemorrhage,
active inflammation, and tissue necrosis with
microabscess formation (Fig. 4). In the three
patients with multiple cavitated nodules, a
variable degree of central necrosis was ob-
served. The inflammatory infiltrate extended
into the surrounding lung parenchyma, and
adjacent areas of hemorrhage were also seen.
Aspergillus colonies were identified within
the lung tissue. Culture confirmation of As-
A B
pergillus fumigatus was obtained in all nine
patients. In one patient, Aspergillus hyphae
were also found in the liver and the gas-
trointestinal tract.
Discussion
Aspergillus organisms are ubiquitous and
are part of the normal environmental flora
that abound in the soil around us. Although
all human beings are commonly exposed to
these organisms, disseminated and invasive
forms of aspergillosis can occur in immuno-
logically compromised hosts [15, 1114].
In severely immunocompromised pa-
tients, invasive pulmonary aspergillosis can
develop [5, 6]. Predisposing factors for the
semiinvasive form of pulmonary aspergillosis
include mildly impaired host immunity and
underlying lung disease. Semiinvasive as-
pergillosis, or chronic necrotizing asper-
gillosis, has radiologic manifestations distinct
C from those of classic invasive aspergillosis [3,
7]. Conditions associated with the develop-
Fig. 2.Semiinvasive aspergillosis in 68-year-old man with chronic bronchitis and recurrent episodes of mild hemoptysis.
A, Thin-section (2-mm collimation) CT scan obtained with lung windows shows rounded area of consolidation
ment of semiinvasive pulmonary aspergillosis
with associated cavitation in left upper lobe. include chronic debilitating illness, diabetes
B, Photograph of left upper lobe pathologic specimen from autopsy shows irregular cavitary lesion with regular mellitus, malnutrition, alcoholism, advanced
margins and dark-brown appearance, consisting of necrotic material and Aspergillus organisms. age, prolonged corticosteroid administration,
C, Photomicrograph of pathologic specimen shows cavitary lesion containing fungal septate hyphae branching
at an acute angle, which is morphologically consistent with aspergillosis. Wall of abscess shows mild inflamma- and chronic obstructive lung disease [3, 7-9].
tory reaction. Surrounding pulmonary parenchyma is healthy. (H and E, 400) Clinical symptoms are often insidious and
AJR:174, January 2000 53
Franquet et al.
Downloaded from www.ajronline.org by 36.78.24.119 on 11/05/14 from IP address 36.78.24.119. Copyright ARRS. For personal use only; all rights reserved
A B
Fig. 3.Multiple bilateral nodules and cavitary aspergillosis in
left upper lobe in 54-year-old man with chronic bronchitis and
recurrent episodes of hemoptysis.
A, Posteroanterior chest radiograph shows multiple nodular
opacities in left lung (straight arrows); paramediastinal ill-de-
fined density is also visible (curved arrow ).
B, Thin-section CT scan confirms presence of bilateral,
multiple, ill-defined nodules of various sizes. Cavitation
with presence of air crescent, not seen on conventional
radiography, was easily shown by CT.
C, Patient died 4 months after CT examination shown in B.
At autopsy, aspergillosis abscesses and multiple small
bronchial and bronchiolar yellowish nodules correspond-
ing to fungal bronchitis were found. Photomicrograph
shows massive Aspergillus hyphae invading bronchial and
bronchiolar epithelium (arrows). (H and E, 400)
C
54 AJR:174, January 2000
Semiinvasive Pulmonary Aspergillosis
Fig. 4.Semiinvasive pulmonary aspergillo-
sis in 56-year-old man with chronic bronchitis
and history of tuberculosis.
A, Posteroanterior chest radiograph obtained 6
months before presentation shows chronic bi-
lateral upper lobe infiltrates with associated
calcified granulomas consistent with previous
tuberculosis (arrows). Perihilar irregular linear
Downloaded from www.ajronline.org by 36.78.24.119 on 11/05/14 from IP address 36.78.24.119. Copyright ARRS. For personal use only; all rights reserved
opacities are also seen.
B, Posteroanterior chest radiograph obtained
at time of presentation shows significant pro-
gression of upper lobe infiltrates.
C, Thin-section CT scan at level of upper lobes
shows bilateral parenchymal consolidation in
both upper lobes.
D, Postmortem microscopic examination con-
firmed fungal infection caused by Aspergillus
fumigatus. Photomicrograph from small area of
consolidation shows tissue necrosis. Aspergil-
lus hyphae (arrows) could be identified in ne-
crotic tissue. (H and E, 400) A B
C D
include chronic cough, sputum production, nonspecific clinical symptoms such as high prevalence of cavitation, occurring in
fever, and constitutional symptoms (weight cough, sputum production, and fever for 53% of lesions, was observed. CT scans
loss and weakness). Hemoptysis is seen in more than 6 months. The slow progression provide accurate information about the ex-
only 15% of patients. of clinical and radiographic findings (several tent and distribution of these cavities and
The diagnosis is often difficult to make be- months to years) may contribute to a delay about the associated pleural thickening. The
cause Aspergillus organisms may be present in in diagnosis [3, 4, 7]. treatment of this form of aspergillosis re-
the sputum or bronchoalveolar lavage fluid in Despite the relatively nonspecific appear- mains controversial; however, good results
patients who have colonization of the airways ance on imaging, unilateral or bilateral pa- have been obtained in symptomatic patients
without tissue invasion [15, 16]. In clinical renchymal opacities in the upper lung zones using IV amphotericin B, oral itraconazole,
practice, the diagnosis of semiinvasive as- are the most common radiographic findings or both.
pergillosis is usually based on the presence of in patients with COPD and semiinvasive as- In conclusion, unilateral or bilateral seg-
multiple cultures positive for Aspergillus or- pergillosis. This upper lobe predominance mental areas of consolidation and multiple
ganisms, chest radiographs with abnormal may be related to the fact that underlying nodular opacities are the most frequent CT
findings, and bronchoscopy biopsy specimens diseased areas of lung promotes this form findings of semiinvasive pulmonary asper-
consistent with tissue invasion. of infection. The findings are similar to gillosis. These findings are nonspecific,
In patients with COPD, semiinvasive as- those seen with tuberculosis. In COPD pa- most commonly mimicking those of reacti-
pergillosis may present with a variety of tients with semiinvasive aspergillosis, a vation tuberculosis.
AJR:174, January 2000 55
Franquet et al.
References study. Radiology 1998;208:777782 drome. N Engl J Med 1991;324:654662
1. Greene R. The pulmonary aspergilloses: three 7. Binder RE, Faling LJ, Pugatch RD, Mahasen C, 12. Brown MJ, Miller RR, Mller NL. Acute lung dis-
distinct entities or a spectrum of disease. Radiol- Snider GL. Chronic necrotizing pulmonary as- ease in the immunocompromised host: CT and
ogy 1981;140:527530 pergillosis: a discrete clinical entity. Medicine pathologic findings. Radiology 1994;190:247254
2. Klein DL, Gamsu G. Thoracic manifestations of 1982;61:109124 13. Logan PM, Mller NL. CT manifestations of pul-
aspergillosis. AJR 1980;134:543552 8. George PJM, Boffa PBJ, Naylor CPE, Higenbottam monary aspergillosis. Crit Rev Diagn Imaging
3. Gefter WB, Weingrad TR, Epstein DM, Ochs RH, TW. Necrotizing pulmonary aspergillosis compli- 1996;37:137
cating the management of patients with obstructive 14. Aquino SL, Kee ST, Warnock ML, Gamsu G.
Downloaded from www.ajronline.org by 36.78.24.119 on 11/05/14 from IP address 36.78.24.119. Copyright ARRS. For personal use only; all rights reserved
Miller WT. Semi-invasive pulmonary as-
pergillosis. Radiology 1981;140:313321 airway disease. Thorax 1983;38:478480 Pulmonary aspergillosis: imaging findings with
4. Gefter WB. The spectrum of pulmonary as- 9. Pittet D, Huguenin T, Dharan S, et al. Unusual cause of pathologic correlation. AJR 1994;163:811815
pergillosis. J Thorac Imaging 1992;7:5674 lethal pulmonary aspergillosis in patients with 15. Yu VL, Muder RR, Porsattar A. Significance of
5. Kuhlman JE, Fishman EK, Siegelman SS. Inva- COPD. Am J Respir Crit Care Med 1996;154:541544 isolation of Aspergillus from the respiratory tract
sive pulmonary aspergillosis in acute leukemia: 10. Saraceno JL, Phelps DT, Ferro TJ, Futerfas R, in diagnosis of invasive pulmonary aspergillosis:
characteristic findings on CT, the CT halo sign, Schwartz DB. Chronic necrotizing pulmonary as- results from a three-year prospective study. Am J
and the role of CT in early diagnosis. Radiology pergillosis: approach and management. Chest Med 1986;81:249254
1985;157:611614 1997;112:541548 16. Treger TR, Visscher DW, Bartlett MS, Smith JW.
6. Won HJ, Lee KS, Cheon JE, et al. Invasive pul- 11. Denning DW, Follansbee SE, Scolaro M, Norris Diagnosis of pulmonary infection caused by As-
monary aspergillosis: prediction at thin section S, Edelstein H, Stevens DA. Pulmonary as- pergillus: usefulness of respiratory cultures. J In-
CT in patients with neutropeniaa prospective pergillosis in the acquired immunodeficiency syn- fect Dis 1985;152:572576
56 AJR:174, January 2000
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Final Case Study - CADDocument109 pagesFinal Case Study - CADPatricia Marie Buenafe100% (1)
- Tonetti Et Al-2018-Journal of Periodontology TDocument14 pagesTonetti Et Al-2018-Journal of Periodontology TJonathan Meza MauricioPas encore d'évaluation
- Grant Jewell Rich Massage Therapy The Evidence For PracticeDocument212 pagesGrant Jewell Rich Massage Therapy The Evidence For PracticeTaune Antonio100% (4)
- Speaking Partner (Meeting 17, Future Plan) WatermarkDocument6 pagesSpeaking Partner (Meeting 17, Future Plan) WatermarkekaPas encore d'évaluation
- Imaging of The Patient With Chronic Bronchitis - An Overview of Old and New Signs - SpringerDocument4 pagesImaging of The Patient With Chronic Bronchitis - An Overview of Old and New Signs - SpringerekaPas encore d'évaluation
- Hemato 1Document8 pagesHemato 1ekaPas encore d'évaluation
- Emfisema PDFDocument7 pagesEmfisema PDFekaPas encore d'évaluation
- CT ScanDocument23 pagesCT ScanekaPas encore d'évaluation
- Category Class Merit Round2 MBBS-BDSDocument102 pagesCategory Class Merit Round2 MBBS-BDSSUSHIL LAKRAPas encore d'évaluation
- Fundamental of Nursing-NleDocument8 pagesFundamental of Nursing-NleJade DigoPas encore d'évaluation
- DR Dina - TB & CovidDocument10 pagesDR Dina - TB & CovidDina FaizahPas encore d'évaluation
- Praktikum Patologi Anatomi: Blok 2.1 Minggu 1 Jejas Sel & InflamasiDocument25 pagesPraktikum Patologi Anatomi: Blok 2.1 Minggu 1 Jejas Sel & Inflamasinawal asmadiPas encore d'évaluation
- DEEP VEIN Dr. Samira BelkheirDocument43 pagesDEEP VEIN Dr. Samira BelkheirkalfPas encore d'évaluation
- Dermatomycological Profile of Patients in A Tertiary Care Hospital of Western MaharashtraDocument2 pagesDermatomycological Profile of Patients in A Tertiary Care Hospital of Western MaharashtraApple IdeaPas encore d'évaluation
- Shingles RecombinantDocument2 pagesShingles Recombinantn99aliPas encore d'évaluation
- 2 NdresearchpaperDocument5 pages2 Ndresearchpaperapi-356685046Pas encore d'évaluation
- A Slice O F: MMR EditionDocument20 pagesA Slice O F: MMR EditionTomTomPas encore d'évaluation
- Oman-Guideline On Good Pharmacovigilance PracticesDocument30 pagesOman-Guideline On Good Pharmacovigilance PracticesAmrPas encore d'évaluation
- Professional PhilosophyDocument8 pagesProfessional Philosophyapi-450228862Pas encore d'évaluation
- RECORDING Form 1: Masterlist of Grade 1 StudentsDocument4 pagesRECORDING Form 1: Masterlist of Grade 1 StudentsGirlie Harical GangawanPas encore d'évaluation
- AJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuDocument7 pagesAJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuYagtaliPas encore d'évaluation
- Proceeding Ilmu KesehatanDocument183 pagesProceeding Ilmu KesehatanIim Rimba100% (1)
- Thyroid Crisis... FinalDocument53 pagesThyroid Crisis... FinalYhanaAdarnePas encore d'évaluation
- Chokde Hudierez - Virtual Hospital Pharmacy Internship JournalDocument5 pagesChokde Hudierez - Virtual Hospital Pharmacy Internship JournalCHOKDE HUDIEREZPas encore d'évaluation
- Rev Plans For 20eb0110 - Provincial HospitalDocument20 pagesRev Plans For 20eb0110 - Provincial HospitalElvin AsanasPas encore d'évaluation
- Catalog Tracoe 2014 PDFDocument94 pagesCatalog Tracoe 2014 PDFLiudmila RailescuPas encore d'évaluation
- Novilyn C. Pataray BSN - Ii Otitis Media: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Otitis Media: St. Paul College of Ilocos SurCharina AubreyPas encore d'évaluation
- Medi Assist Policy Conditions 2018-19Document22 pagesMedi Assist Policy Conditions 2018-19saran2rasuPas encore d'évaluation
- Jurnal Manajemen Apotek PDFDocument11 pagesJurnal Manajemen Apotek PDFAlexSiNagaPas encore d'évaluation
- Sephan Eve-In - Intensive - Care - Transport - VentilationDocument4 pagesSephan Eve-In - Intensive - Care - Transport - VentilationzorgglubPas encore d'évaluation
- Emotion and Personality in Health and HealthcareDocument6 pagesEmotion and Personality in Health and HealthcareElena-Andreea MutPas encore d'évaluation
- (PDF) Diabetes Causes, Symptoms and TreatmentsDocument1 page(PDF) Diabetes Causes, Symptoms and TreatmentsBakaro ShafiPas encore d'évaluation
- Will Maclean - Clinical Handbook of Chinese Herbs - Desk Reference, Revised Edition-Singing Dragon (2017)Document170 pagesWill Maclean - Clinical Handbook of Chinese Herbs - Desk Reference, Revised Edition-Singing Dragon (2017)amitlkoyogaPas encore d'évaluation
- Animal Testing: Pros and ConsDocument11 pagesAnimal Testing: Pros and ConsabhishekjainitPas encore d'évaluation
- Pathophysiology Schematic Diagram and NarrativeDocument15 pagesPathophysiology Schematic Diagram and NarrativeKathrina CravePas encore d'évaluation