Vous aimerez peut-être aussi
- Ehab 268Document2 pagesEhab 268yori yarson tonPas encore d'évaluation
- JCVTR 6 35Document7 pagesJCVTR 6 35christ_cruzerPas encore d'évaluation
- Arrhytmia in ICUDocument2 pagesArrhytmia in ICUEvita FebriyantiPas encore d'évaluation
- Cardiology: Risk Stratification in Brugada Syndrome: Role of Programmed Electrical StimulationDocument4 pagesCardiology: Risk Stratification in Brugada Syndrome: Role of Programmed Electrical StimulationIke AdrianaPas encore d'évaluation
- Usefulness of Diabetes Mellitus To Predict Long-Term Outcomes in Patients With Unstable Angina Pectoris.Document15 pagesUsefulness of Diabetes Mellitus To Predict Long-Term Outcomes in Patients With Unstable Angina Pectoris.Diah Kris AyuPas encore d'évaluation
- Endocarditis in The Elderly: Clinical, Echocardiographic, and Prognostic FeaturesDocument8 pagesEndocarditis in The Elderly: Clinical, Echocardiographic, and Prognostic FeaturesMehdi285858Pas encore d'évaluation
- Case Series - Acute Coronary SyndromeDocument18 pagesCase Series - Acute Coronary SyndromenikPas encore d'évaluation
- Vital Signs Are UnreliableDocument3 pagesVital Signs Are UnreliablemediclassroomPas encore d'évaluation
- 2022 Clinical Features and Risk Factors of Mortality in Patients With Posterior Reversible Encephalopathy SyndromeDocument7 pages2022 Clinical Features and Risk Factors of Mortality in Patients With Posterior Reversible Encephalopathy SyndromeSafitri MuhlisaPas encore d'évaluation
- Journal - Pone.0105785 AMI&ACIDocument9 pagesJournal - Pone.0105785 AMI&ACILidya ChristyPas encore d'évaluation
- ABO Blood Groups As A Disease Marker To Predict atDocument12 pagesABO Blood Groups As A Disease Marker To Predict atMohammad Mohammad MohammedPas encore d'évaluation
- Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 DiabetesDocument12 pagesEmpagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 DiabetesVh TRPas encore d'évaluation
- Castle AfDocument11 pagesCastle AfgustavoPas encore d'évaluation
- Stroke PDFDocument67 pagesStroke PDFBadrul MunirPas encore d'évaluation
- Natural History of Asymptomatic Severe Aortic StenosisDocument11 pagesNatural History of Asymptomatic Severe Aortic StenosisGaal PinPas encore d'évaluation
- Retrospective Study of Elderly Frequent Attenders Presenting With Chest Pain at Emergency DepartmentDocument5 pagesRetrospective Study of Elderly Frequent Attenders Presenting With Chest Pain at Emergency DepartmentrantiningsihsumarniPas encore d'évaluation
- Seiffge 2018Document3 pagesSeiffge 2018barti koksPas encore d'évaluation
- Eficacia de La Telemedicina en El Manejo de La Insuficiencia CardíacaDocument11 pagesEficacia de La Telemedicina en El Manejo de La Insuficiencia CardíacaSMIBA MedicinaPas encore d'évaluation
- Life 11 01429Document14 pagesLife 11 01429Genesis PerezPas encore d'évaluation
- 2001 - Value of ECG in AMI - JAMADocument8 pages2001 - Value of ECG in AMI - JAMAMichail PapafaklisPas encore d'évaluation
- Predicting The Risk For Dialysis or Death in Iga NephropathyDocument10 pagesPredicting The Risk For Dialysis or Death in Iga Nephropathyjustin_sanePas encore d'évaluation
- J Thromres 2012 05 016Document6 pagesJ Thromres 2012 05 016Alexandra RosaPas encore d'évaluation
- Atrial FibrillationDocument18 pagesAtrial FibrillationmamaluPas encore d'évaluation
- In Hospital Cardiac Complications After Intracerebral HemorrhageDocument6 pagesIn Hospital Cardiac Complications After Intracerebral HemorrhageIdrianaPas encore d'évaluation
- Af Prevention CHFDocument4 pagesAf Prevention CHFDewi AyuPas encore d'évaluation
- Journal 4Document7 pagesJournal 4Denys PutraPas encore d'évaluation
- Eurheartj Ehu357 FullDocument8 pagesEurheartj Ehu357 FullagneselimPas encore d'évaluation
- FMZ 020Document6 pagesFMZ 020octawyanaPas encore d'évaluation
- Association of Proteinuria and Incident Atrial Fibrillation in Patients With Diabetes Mellitus: A Population Based Senior Cohort StudyDocument10 pagesAssociation of Proteinuria and Incident Atrial Fibrillation in Patients With Diabetes Mellitus: A Population Based Senior Cohort StudydrkhengkiPas encore d'évaluation
- Long Term Mortality of Deep Sternal Wound Infection After Coronary Artery Bypass SurgeryDocument6 pagesLong Term Mortality of Deep Sternal Wound Infection After Coronary Artery Bypass SurgeryMartha CeciliaPas encore d'évaluation
- Prognosis and Monitoring of VTEDocument13 pagesPrognosis and Monitoring of VTEYohanaSidabalokPas encore d'évaluation
- High Blood Pressure in Patients With Prader Willi Syndrome: Case Report and Review of The LiteratureDocument3 pagesHigh Blood Pressure in Patients With Prader Willi Syndrome: Case Report and Review of The LiteratureIJAR JOURNALPas encore d'évaluation
- Comment: Vs 140 (61 4%) of 228 Patients Hazard Ratio (HR)Document2 pagesComment: Vs 140 (61 4%) of 228 Patients Hazard Ratio (HR)Barbara Sakura RiawanPas encore d'évaluation
- Clinical Features and Outcomes of Takotsubo Stress Cardiomyopathy NEJMoa1406761Document10 pagesClinical Features and Outcomes of Takotsubo Stress Cardiomyopathy NEJMoa1406761William LeePas encore d'évaluation
- 1 s2.0 S0735109710020851 MainDocument11 pages1 s2.0 S0735109710020851 Mainblooom_00Pas encore d'évaluation
- Estudio Electrofisiológico Con Marcapasos Profiláctico y Supervivencia en DM.Document10 pagesEstudio Electrofisiológico Con Marcapasos Profiláctico y Supervivencia en DM.El ArcangelPas encore d'évaluation
- 6 Antithrombotic Therapy in Patients With Infective EndocarditisDocument12 pages6 Antithrombotic Therapy in Patients With Infective Endocarditisabdeali hazariPas encore d'évaluation
- Journal 1Document39 pagesJournal 1armeliaPas encore d'évaluation
- Heart 2002 Menon 531 7Document8 pagesHeart 2002 Menon 531 7TriponiaPas encore d'évaluation
- Cryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekDocument8 pagesCryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekferrevPas encore d'évaluation
- Accidente Cerebrovascular Criptogénico Yforamen Oval Permea 2018Document9 pagesAccidente Cerebrovascular Criptogénico Yforamen Oval Permea 2018federico saldariniPas encore d'évaluation
- The Role of Cardiac Troponin I in Prognostication of Patients With Isolated Severe Traumatic Brain InjuryDocument7 pagesThe Role of Cardiac Troponin I in Prognostication of Patients With Isolated Severe Traumatic Brain InjuryMarizaPas encore d'évaluation
- Atrial Fibrillation As The Cause of Reccurent TIA in Young Female Adult FinalDocument2 pagesAtrial Fibrillation As The Cause of Reccurent TIA in Young Female Adult FinalNathania HoswandiPas encore d'évaluation
- Catheter Ablationin in AF With CHFDocument11 pagesCatheter Ablationin in AF With CHFKristian Sudana HartantoPas encore d'évaluation
- Bradyarrhythmias in Patientswith COVID-19Document6 pagesBradyarrhythmias in Patientswith COVID-19Marcela Soruco AyupePas encore d'évaluation
- Dichotomizing High-Sensitivity Cardiac Troponin T Results and Important Analytical ConsiderationsDocument2 pagesDichotomizing High-Sensitivity Cardiac Troponin T Results and Important Analytical ConsiderationsIvanaPas encore d'évaluation
- Clinical Characteristics, PrecDocument12 pagesClinical Characteristics, PrecSiti ArwaniPas encore d'évaluation
- Neshige 2015Document5 pagesNeshige 2015belleswanPas encore d'évaluation
- Atrial Fibrillation - Annals of Internal Medicine (2023)Document18 pagesAtrial Fibrillation - Annals of Internal Medicine (2023)silvermist100% (2)
- Race Ii 2010 NejmDocument11 pagesRace Ii 2010 NejmAxel Hiram Hernandez PinedaPas encore d'évaluation
- Milri Vs DobutaDocument10 pagesMilri Vs DobutaEliana Lopez BaronPas encore d'évaluation
- Article - Facteurs Pronostiques de L'insuffisance CardiaqueDocument1 pageArticle - Facteurs Pronostiques de L'insuffisance CardiaqueAbdoul Nasser GarbaPas encore d'évaluation
- Bernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?Document26 pagesBernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?om mkPas encore d'évaluation
- Articulo Suplementos en Pacientes Contacto TBDocument16 pagesArticulo Suplementos en Pacientes Contacto TBstephanie bojorquezPas encore d'évaluation
- Acute Heart Failure Syndromes: Mihai Gheorghiade, MD, FACC, Peter S. Pang, MDDocument17 pagesAcute Heart Failure Syndromes: Mihai Gheorghiade, MD, FACC, Peter S. Pang, MDcornelyPas encore d'évaluation
- WNL 0000000000000176Document3 pagesWNL 0000000000000176Nona Suci rahayuPas encore d'évaluation
- 2018 Nyeri ACS VinsurDocument11 pages2018 Nyeri ACS VinsurriniPas encore d'évaluation
- Cardiac Complications in Diphtheria and Predictors of OutcomesDocument12 pagesCardiac Complications in Diphtheria and Predictors of OutcomesPratiwi Indah PalupiPas encore d'évaluation
- 1212 Full PDFDocument9 pages1212 Full PDFChris KronzPas encore d'évaluation
- Clinical Approach to Sudden Cardiac Death SyndromesD'EverandClinical Approach to Sudden Cardiac Death SyndromesRamon BrugadaPas encore d'évaluation
- Skuy LaDocument7 pagesSkuy LaAnonymous 7dsX2F8nPas encore d'évaluation
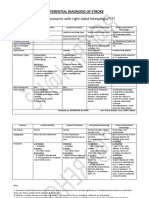
- Differential Diagnosis of StrokeDocument2 pagesDifferential Diagnosis of StrokeAnonymous 7dsX2F8nPas encore d'évaluation
- AsuasuasususuDocument67 pagesAsuasuasususuAnonymous 7dsX2F8nPas encore d'évaluation
- Exercise Training For Blood Pressure: A Systematic Review and Meta-AnalysisDocument9 pagesExercise Training For Blood Pressure: A Systematic Review and Meta-AnalysisAnonymous 7dsX2F8nPas encore d'évaluation
- Therapeutic Use of Stem Cells in Treatment of Burn Injuries: Summary ArticleDocument8 pagesTherapeutic Use of Stem Cells in Treatment of Burn Injuries: Summary ArticleAnonymous 7dsX2F8nPas encore d'évaluation
- ISMKI InductionDocument19 pagesISMKI InductionAnonymous 7dsX2F8nPas encore d'évaluation
- Film RecomendDocument1 pageFilm RecomendAnonymous 7dsX2F8nPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptAnonymous 7dsX2F8nPas encore d'évaluation
- Journal of Computational and Applied Mathematics: M. Filomena Teodoro, Carla SimãoDocument7 pagesJournal of Computational and Applied Mathematics: M. Filomena Teodoro, Carla SimãoAnonymous 7dsX2F8nPas encore d'évaluation
- Etiologi & Penatalaksanaan Dub: Erald Giovanny Hasiholan Simatupang FAA 115 027Document6 pagesEtiologi & Penatalaksanaan Dub: Erald Giovanny Hasiholan Simatupang FAA 115 027Anonymous 7dsX2F8nPas encore d'évaluation
- Acute Diarrhea in AdultsDocument2 pagesAcute Diarrhea in AdultsAnonymous 7dsX2F8nPas encore d'évaluation
- Heart Failure: Preventing Disease and Death WorldwideDocument39 pagesHeart Failure: Preventing Disease and Death WorldwideAnonymous 7dsX2F8nPas encore d'évaluation
- Read MeyppppppppppppppoooooDocument2 pagesRead MeyppppppppppppppoooooAnonymous 7dsX2F8nPas encore d'évaluation
- Inborn Errors or MetabolismDocument25 pagesInborn Errors or MetabolismAnonymous 7dsX2F8nPas encore d'évaluation
- Kjim 2016 098Document9 pagesKjim 2016 098Anonymous 7dsX2F8nPas encore d'évaluation
- CL Analyzer: Coagulometric, Chromogenic and Immunological AssaysDocument2 pagesCL Analyzer: Coagulometric, Chromogenic and Immunological AssaysEdwinPas encore d'évaluation
- SRV SLB222 en - 05062020Document2 pagesSRV SLB222 en - 05062020Nguyen ThuongPas encore d'évaluation
- BS7-Touch Screen PanelDocument96 pagesBS7-Touch Screen PanelEduardo Diaz Pichardo100% (1)
- Distribución Del Mercurio Total en Pescados y Mariscos Del Mar ArgentinoDocument15 pagesDistribución Del Mercurio Total en Pescados y Mariscos Del Mar ArgentinoaldiPas encore d'évaluation
- Imagine Unit 1 P 10 11Document1 pageImagine Unit 1 P 10 11נויה לבדובPas encore d'évaluation
- Installation Manual (DH84309201) - 07Document24 pagesInstallation Manual (DH84309201) - 07mquaiottiPas encore d'évaluation
- Cash and Cash Equivalents ReviewerDocument4 pagesCash and Cash Equivalents ReviewerEileithyia KijimaPas encore d'évaluation
- Aseptic TechniquesDocument3 pagesAseptic TechniquesMacy MarianPas encore d'évaluation
- EDC MS5 In-Line Injection Pump: Issue 2Document57 pagesEDC MS5 In-Line Injection Pump: Issue 2Musharraf KhanPas encore d'évaluation
- Marine Advisory 03-22 LRITDocument2 pagesMarine Advisory 03-22 LRITNikos StratisPas encore d'évaluation
- Bakery Ind HygieneDocument104 pagesBakery Ind Hygienelabie100% (1)
- Pakeha (Maori For European New Zealanders) Thinking, in That They Tend To Go OutwardsDocument11 pagesPakeha (Maori For European New Zealanders) Thinking, in That They Tend To Go OutwardsDwi RahayuPas encore d'évaluation
- Astm A712 PDFDocument3 pagesAstm A712 PDFCristian OtivoPas encore d'évaluation
- AcquaculturaDocument145 pagesAcquaculturamidi64100% (1)
- Quarterly Progress Report FormatDocument7 pagesQuarterly Progress Report FormatDegnesh AssefaPas encore d'évaluation
- 0010 kOBELCO SK 179-9 PDFDocument52 pages0010 kOBELCO SK 179-9 PDFDaman Huri100% (2)
- The Chemical Composition and Organoleptic Attributes of Lesser-Known Vegetables As Consumed in Njikoka Local Government Area, Anambra State, NigeriaDocument4 pagesThe Chemical Composition and Organoleptic Attributes of Lesser-Known Vegetables As Consumed in Njikoka Local Government Area, Anambra State, NigeriaEmri CynthiaPas encore d'évaluation
- Presentation of DR Rai On Sahasrara Day Medical SessionDocument31 pagesPresentation of DR Rai On Sahasrara Day Medical SessionRahul TikkuPas encore d'évaluation
- DIAC Experienced Associate HealthcareDocument3 pagesDIAC Experienced Associate HealthcarecompangelPas encore d'évaluation
- RCM Design and ImplementationDocument34 pagesRCM Design and ImplementationRozi YudaPas encore d'évaluation
- Mental Status ExaminationDocument34 pagesMental Status Examinationkimbomd100% (2)
- Universal Robina Sugar Milling Vs AciboDocument7 pagesUniversal Robina Sugar Milling Vs AciboCeresjudicataPas encore d'évaluation
- TelfastDocument3 pagesTelfastjbahalkehPas encore d'évaluation
- INTELLECTUAL DISABILITY NotesDocument6 pagesINTELLECTUAL DISABILITY Notesshai gestPas encore d'évaluation
- ME-317 Internal Combustion Engines - TurbochargingDocument21 pagesME-317 Internal Combustion Engines - TurbochargingHamzaJavedPas encore d'évaluation
- Ammonium Chloride: Product InformationDocument2 pagesAmmonium Chloride: Product InformationusamaPas encore d'évaluation
- BlackCat ManualDocument14 pagesBlackCat ManualNestor Marquez-DiazPas encore d'évaluation
- Brachiocephalic TrunkDocument3 pagesBrachiocephalic TrunkstephPas encore d'évaluation
- 2017 THE BLUE WAY Visual PDFDocument54 pages2017 THE BLUE WAY Visual PDFAlex KappelPas encore d'évaluation
- API 614-Chapter 4 DATA SHEET Dry Gas Seal Module Si Units: System Responsibility: (2.1.2)Document10 pagesAPI 614-Chapter 4 DATA SHEET Dry Gas Seal Module Si Units: System Responsibility: (2.1.2)tutuionutPas encore d'évaluation