Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Journal Reading Genitourinary Syndrome of Menopouse: An Overview of Clinical Manifestations, Pathophysiology, Etiology, Evaluation, and ManagementDocument1 pageJournal Reading Genitourinary Syndrome of Menopouse: An Overview of Clinical Manifestations, Pathophysiology, Etiology, Evaluation, and ManagementGorindraPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Final PMDK 2012Document14 pagesFinal PMDK 2012GorindraPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Instrumentsusedingynecologyandobstetricsyoungdoctorsresearchforum 141213031922 Conversion Gate02Document16 pagesInstrumentsusedingynecologyandobstetricsyoungdoctorsresearchforum 141213031922 Conversion Gate02GorindraPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Journal Reading 3Document8 pagesJournal Reading 3GorindraPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- JurnalDocument6 pagesJurnalGorindraPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Nucleus Pulposus-Induced Nerve Root Injury: Effects of Diclofenac and KetoprofenDocument6 pagesNucleus Pulposus-Induced Nerve Root Injury: Effects of Diclofenac and KetoprofenGorindraPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Operative Gyn MCQ PDFDocument10 pagesOperative Gyn MCQ PDFFentahun TadessePas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Gastric Cancer in The East and West What Should We LearnDocument1 pageGastric Cancer in The East and West What Should We LearnBrahim OuyabaPas encore d'évaluation
- Urinary SystemDocument9 pagesUrinary SystemCailah Sofia SelausoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- 3, 4: Circulatory Disturbance: Patum (K3 - K4)Document8 pages3, 4: Circulatory Disturbance: Patum (K3 - K4)Anna TohPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- UROLOGIADocument117 pagesUROLOGIAestefanyao1Pas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Development of MandibleDocument60 pagesDevelopment of MandibleAlisha Aranha100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Cataract Surgery Side EffectsDocument4 pagesCataract Surgery Side EffectsEye spacialistPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Kea-Med Medical College 22 Campus: Title: Family Planning Project Work Surgical Contraceptive Individual AssignmentDocument13 pagesKea-Med Medical College 22 Campus: Title: Family Planning Project Work Surgical Contraceptive Individual AssignmentlahmetoPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Fasting or Starving Our Patients To An Inhumane Extent? A Plea For Some Common SenseDocument3 pagesFasting or Starving Our Patients To An Inhumane Extent? A Plea For Some Common SenseRajesh GyawaliPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- AOFASDocument5 pagesAOFASAlessandro MedinaPas encore d'évaluation
- Colon, Rectum & AnusDocument6 pagesColon, Rectum & AnusLeikkaPas encore d'évaluation
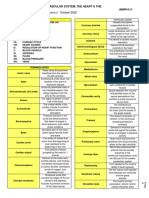
- 1.08 - The Cardiovascular System, The Heart & The Blood VesselsDocument9 pages1.08 - The Cardiovascular System, The Heart & The Blood Vessels13PLAN, SENTH RUEN, APas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- New Microsoft Office PowerPoint PresentationDocument33 pagesNew Microsoft Office PowerPoint PresentationVasuda Devi MalepatiPas encore d'évaluation
- Acromioclavicular and Sternoclavicular Joint SprainDocument6 pagesAcromioclavicular and Sternoclavicular Joint Sprainlsrys1130Pas encore d'évaluation
- The Swing Lock Denture Its Use in Conventional Removable Partial Denture Prosthodontics PDFDocument3 pagesThe Swing Lock Denture Its Use in Conventional Removable Partial Denture Prosthodontics PDFscott_c_kane100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Art of PhacoemulsificationDocument544 pagesThe Art of PhacoemulsificationDaniel Fernández Gajardo100% (3)
- Abdominal Examination Check ListDocument9 pagesAbdominal Examination Check ListIbrahim Ahmed IbrahimPas encore d'évaluation
- 0 Endocon 202Document53 pages0 Endocon 202AliabdulghaniPas encore d'évaluation
- DAFTAR PUSTAKA YuniiiDocument3 pagesDAFTAR PUSTAKA Yuniiiule kenziPas encore d'évaluation
- Groupd Ebp PresentationDocument38 pagesGroupd Ebp Presentationapi-384226081Pas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- TracheotomyDocument4 pagesTracheotomyWilma VeniaPas encore d'évaluation
- 2.2 Medical Surgical Nursing - II QPDocument16 pages2.2 Medical Surgical Nursing - II QPAnju Karunakaran100% (1)
- The Ulnar Collateral Ligament InjuryDocument11 pagesThe Ulnar Collateral Ligament InjuryMarisé Llanos RoblesPas encore d'évaluation
- System Brochure - Fusion Cup System PDFDocument4 pagesSystem Brochure - Fusion Cup System PDFAngulo HernandezPas encore d'évaluation
- 4 6006056625771644091Document11 pages4 6006056625771644091King GeorgePas encore d'évaluation
- 9 Odontogenic Infections and Pyogenic Infections of The Soft TissuesDocument9 pages9 Odontogenic Infections and Pyogenic Infections of The Soft Tissuesاحمد سلامPas encore d'évaluation
- Optilube Brochure 2012Document4 pagesOptilube Brochure 2012Optimum Medical SolutionsPas encore d'évaluation
- Accidental Intra Arterial Injection Joel ArudchelvamDocument3 pagesAccidental Intra Arterial Injection Joel ArudchelvamJoel Arudchelvam100% (1)
- CastDocument7 pagesCastRegina Nina YoshidaPas encore d'évaluation
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)