Vous aimerez peut-être aussi
- MRCPCH Clinical: Short Cases, History Taking & Communication Skills 3eDocument19 pagesMRCPCH Clinical: Short Cases, History Taking & Communication Skills 3ePasTestBooks100% (6)
- RACP Long Case Notes Boutlis 2014Document7 pagesRACP Long Case Notes Boutlis 2014Gus LionsPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Mosco's Clerking Guide..Document88 pagesMosco's Clerking Guide..temitopePas encore d'évaluation
- SOAP Note AdviceDocument5 pagesSOAP Note AdviceNico AvellanaPas encore d'évaluation
- History of Present IllnessDocument10 pagesHistory of Present Illnesshirsi200518Pas encore d'évaluation
- A Road Map For The Soap Note-2021-2022: Name: DobDocument3 pagesA Road Map For The Soap Note-2021-2022: Name: DobDat Phan100% (1)
- ATSP Booklet 2023Document26 pagesATSP Booklet 2023Savanthi Carmaline de SilvaPas encore d'évaluation
- A Practical Guide To Clinical MedicineDocument5 pagesA Practical Guide To Clinical Medicinejjj100% (3)
- Scut PuppyDocument68 pagesScut Puppysgod34Pas encore d'évaluation
- Positive Options for Antiphospholipid Syndrome (APS): Self-Help and TreatmentD'EverandPositive Options for Antiphospholipid Syndrome (APS): Self-Help and TreatmentÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- 0 MnemonicsDocument133 pages0 MnemonicsAlex Ivan Chen TejadaPas encore d'évaluation
- Postoperative Care in Thoracic Surgery A Comprehensive GuideDocument397 pagesPostoperative Care in Thoracic Surgery A Comprehensive GuideΑΘΑΝΑΣΙΟΣ ΚΟΥΤΟΥΚΤΣΗΣ100% (1)
- Chomp Excersie 3Document5 pagesChomp Excersie 3Omahri24Pas encore d'évaluation
- Passing 3rd Year at University College London Medical SchoolDocument6 pagesPassing 3rd Year at University College London Medical Schoolkjb57Pas encore d'évaluation
- House JobDocument177 pagesHouse Jobwalasr83Pas encore d'évaluation
- Triage and Priority SettingDocument10 pagesTriage and Priority SettingekonurcahyaningrumPas encore d'évaluation
- Resident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)Document104 pagesResident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)scalixto100% (1)
- Practical Guide To Common ENT On-Call Problems in Edmonton, ABDocument43 pagesPractical Guide To Common ENT On-Call Problems in Edmonton, ABdentaldudecalPas encore d'évaluation
- 9 Tips On How To Make A Good SOAPIEDocument4 pages9 Tips On How To Make A Good SOAPIEShara SampangPas encore d'évaluation
- Carte Anamneza Si TestareDocument100 pagesCarte Anamneza Si TestareNarcis PopaPas encore d'évaluation
- Surgery Tips and ResourcesDocument2 pagesSurgery Tips and ResourcesAbeebs SalahouPas encore d'évaluation
- PhiDocument11 pagesPhiGitaq Tri YatmaPas encore d'évaluation
- PANCE or PANRE PA Exam What Do Zebras Have To Do With My SuccessDocument2 pagesPANCE or PANRE PA Exam What Do Zebras Have To Do With My SuccessHELP PANCE PANRE Online PA Exam Review CoursePas encore d'évaluation
- Cara Menulis CAse ClerkingDocument4 pagesCara Menulis CAse ClerkingShi Kin LauPas encore d'évaluation
- NEUROPrelims - History Taking in NeurologyDocument4 pagesNEUROPrelims - History Taking in NeurologyRenatoCosmeGalvanJuniorPas encore d'évaluation
- Why I Let My Patients See My NotesDocument2 pagesWhy I Let My Patients See My NotesRanoCenterPas encore d'évaluation
- Determination of DeathDocument14 pagesDetermination of DeathIlyes FerenczPas encore d'évaluation
- Whatcom County EMT BLS Transport ProgramDocument85 pagesWhatcom County EMT BLS Transport ProgramdadaditdahPas encore d'évaluation
- Chapter 2: History TakingDocument11 pagesChapter 2: History TakingHo Yong WaiPas encore d'évaluation
- 9 Tips On How To Make A Good SOAPIEDocument7 pages9 Tips On How To Make A Good SOAPIEMagbanua Airene MarielPas encore d'évaluation
- Presenting Your Patient: A Guide For Medical Students Rotating in The Emergency Department (Tamara Howard, MD Kerry B Broderick, MD)Document7 pagesPresenting Your Patient: A Guide For Medical Students Rotating in The Emergency Department (Tamara Howard, MD Kerry B Broderick, MD)jroshsperlingPas encore d'évaluation
- HEENT History TakingDocument15 pagesHEENT History TakingPépé TechopathamPas encore d'évaluation
- OSCE S BibleDocument66 pagesOSCE S BibleApoorva SaxenaPas encore d'évaluation
- Adult NAC RevisedDocument26 pagesAdult NAC RevisedOsan BogdanPas encore d'évaluation
- A. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherDocument70 pagesA. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherMwansaay Twain HolyPas encore d'évaluation
- ClaseMagisterCorazon09 05 2021 01 29 01.mp3Document5 pagesClaseMagisterCorazon09 05 2021 01 29 01.mp3Jonas BlackPas encore d'évaluation
- Interview QuestionsDocument7 pagesInterview QuestionsMuhammad SaadPas encore d'évaluation
- Clinical Decision MakingDocument7 pagesClinical Decision MakingPablo Eduardo AmadorPas encore d'évaluation
- (ED, Our Service Etc) Complaining of - We Were Consulted ForDocument5 pages(ED, Our Service Etc) Complaining of - We Were Consulted ForGaetano Di GiovanniPas encore d'évaluation
- L: Listening E: Eliciting Info G: Giving Info R: Respectful E: Empathetic P: ProfessionalDocument3 pagesL: Listening E: Eliciting Info G: Giving Info R: Respectful E: Empathetic P: ProfessionalSolomon Seth SallforsPas encore d'évaluation
- Med#1Document9 pagesMed#1api-3855312Pas encore d'évaluation
- Slide 1 H & P For Dental StudentDocument45 pagesSlide 1 H & P For Dental StudentPrince AhmedPas encore d'évaluation
- How To Talk About Illness and Medicine in EnglishDocument5 pagesHow To Talk About Illness and Medicine in EnglishIsmaPas encore d'évaluation
- Echocardiography Beyond the First Clinical Scenarios: A Guide for Your First JobD'EverandEchocardiography Beyond the First Clinical Scenarios: A Guide for Your First JobPas encore d'évaluation
- Tugas Medical English IiDocument3 pagesTugas Medical English IiAsridewi DewiPas encore d'évaluation
- History Taking NotesDocument7 pagesHistory Taking NotesZWEASPas encore d'évaluation
- The Rubik's Cube Approach To Clinical MedicineDocument2 pagesThe Rubik's Cube Approach To Clinical Medicinehenrygoldstein100% (1)
- History and Physical Examination: Medical ProfessionalsDocument10 pagesHistory and Physical Examination: Medical ProfessionalsGiorgio CivitaresePas encore d'évaluation
- Internal Medicine NotesDocument271 pagesInternal Medicine NotesMUNNA shaik100% (1)
- The Art of Patient PresentationsDocument24 pagesThe Art of Patient Presentationsminerva_stanciuPas encore d'évaluation
- Transcript FDMT 5241Document32 pagesTranscript FDMT 5241juliana izquierdoPas encore d'évaluation
- Meded Guidelines Oral PresentationsDocument12 pagesMeded Guidelines Oral PresentationsIqra JanjuaPas encore d'évaluation
- HOPI in History TakingDocument5 pagesHOPI in History TakingKumar KP100% (1)
- The Medical History: Herni SupraptiDocument101 pagesThe Medical History: Herni SupraptiPradika Abdi PutraPas encore d'évaluation
- Clerking 101Document7 pagesClerking 101Parsaant SinghPas encore d'évaluation
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyPas encore d'évaluation
- Tally and O'Connor's Clinical Examination (8 Edition, Volume 1) Notes & Summaries by Yasin KadriDocument9 pagesTally and O'Connor's Clinical Examination (8 Edition, Volume 1) Notes & Summaries by Yasin KadriYasin KadriPas encore d'évaluation
- MRCGP OsceDocument17 pagesMRCGP OsceJaved Yakoob100% (1)
- Nursing Comps Study GuideDocument15 pagesNursing Comps Study GuideforminskoPas encore d'évaluation
- Clerking 101Document8 pagesClerking 101Adil IslamPas encore d'évaluation
- Clinical Case Presentations CARE IIDocument44 pagesClinical Case Presentations CARE IIStarr Newman100% (1)
- Transcription: 13 Jan Session 2 - Recording - 1Document4 pagesTranscription: 13 Jan Session 2 - Recording - 1David ValbuenaPas encore d'évaluation
- Lecturio ComDocument7 pagesLecturio ComAlex Ivan Chen TejadaPas encore d'évaluation
- LAws of House of AnovaDocument2 pagesLAws of House of AnovaAlex Ivan Chen TejadaPas encore d'évaluation
- Urinary Incontinence Barone CheatsheetDocument1 pageUrinary Incontinence Barone CheatsheetimprazePas encore d'évaluation
- Alcohol Poisoning Cheatsheet PDFDocument1 pageAlcohol Poisoning Cheatsheet PDFAlex Ivan Chen TejadaPas encore d'évaluation
- Mnemonics For Bio, MicroDocument9 pagesMnemonics For Bio, MicroAlex Ivan Chen TejadaPas encore d'évaluation
- Common Intestinal Helminths of Man: Life Cycle ChartsDocument32 pagesCommon Intestinal Helminths of Man: Life Cycle ChartsAlex Ivan Chen TejadaPas encore d'évaluation
- Intestinal ProtozoaDocument25 pagesIntestinal ProtozoaAlex Ivan Chen TejadaPas encore d'évaluation
- Online Games and Academic AchievementDocument25 pagesOnline Games and Academic AchievementJasmine GamoraPas encore d'évaluation
- Section 80CCD (1B) Deduction - About NPS Scheme & Tax BenefitsDocument7 pagesSection 80CCD (1B) Deduction - About NPS Scheme & Tax BenefitsP B ChaudharyPas encore d'évaluation
- English PoemDocument4 pagesEnglish Poemapi-276985258Pas encore d'évaluation
- Boeco BM-800 - User ManualDocument21 pagesBoeco BM-800 - User ManualJuan Carlos CrespoPas encore d'évaluation
- Constantino V MendezDocument3 pagesConstantino V MendezNīc CādīgālPas encore d'évaluation
- PulpectomyDocument3 pagesPulpectomyWafa Nabilah Kamal100% (1)
- MCQ Homework: PeriodonticsDocument4 pagesMCQ Homework: Periodonticsفراس الموسويPas encore d'évaluation
- CFPB Discount Points Guidence PDFDocument3 pagesCFPB Discount Points Guidence PDFdzabranPas encore d'évaluation
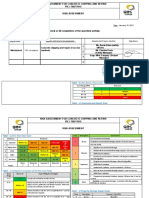
- Ra Concrete Chipping 7514Document5 pagesRa Concrete Chipping 7514Charles DoriaPas encore d'évaluation
- Case Report 3 MukokelDocument3 pagesCase Report 3 MukokelWidychii GadiestchhetyaPas encore d'évaluation
- Menu Siklus RSDocument3 pagesMenu Siklus RSChika VionitaPas encore d'évaluation
- (Engine International Air Pollution Prevention) : EIAPP CertificateDocument2 pages(Engine International Air Pollution Prevention) : EIAPP CertificateTan DatPas encore d'évaluation
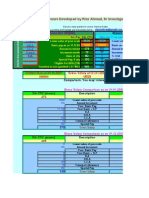
- Emission Estimation Technique Manual: For Mining and Processing of Non-Metallic MineralsDocument84 pagesEmission Estimation Technique Manual: For Mining and Processing of Non-Metallic MineralsAbdelaziem mahmoud abdelaalPas encore d'évaluation
- Sol. Mock Test CBSE BiologyDocument3 pagesSol. Mock Test CBSE BiologysbarathiPas encore d'évaluation
- Tcu Module Pe1 Lesson 1Document7 pagesTcu Module Pe1 Lesson 1Remerata, ArcelynPas encore d'évaluation
- ANATOMY 1 NILEM and Cat FISHDocument19 pagesANATOMY 1 NILEM and Cat FISHAnisatul Khabibah ZaenPas encore d'évaluation
- Safety AuditDocument9 pagesSafety AuditRobena Nagum BagasPas encore d'évaluation
- EF4e Beg Quicktest 05Document3 pagesEF4e Beg Quicktest 05terrenoruralcamboriuPas encore d'évaluation
- Biodegradable Plastic Bag Manufacturing Industry-800655 PDFDocument68 pagesBiodegradable Plastic Bag Manufacturing Industry-800655 PDFAryanPas encore d'évaluation
- Packed Bed Reactor Slides (B)Document32 pagesPacked Bed Reactor Slides (B)Meireza Ajeng PratiwiPas encore d'évaluation
- 8 Categories of Lipids: FunctionsDocument3 pages8 Categories of Lipids: FunctionsCaryl Alvarado SilangPas encore d'évaluation
- The Problem of Units and The Circumstance For POMPDocument33 pagesThe Problem of Units and The Circumstance For POMPamarendra123Pas encore d'évaluation
- Mdp36 The EndDocument42 pagesMdp36 The Endnanog36Pas encore d'évaluation
- Rigging: GuideDocument244 pagesRigging: Guideyusry72100% (11)
- EB Research Report 2011Document96 pagesEB Research Report 2011ferlacunaPas encore d'évaluation
- Pressure Vessels SHO ProgrammeDocument42 pagesPressure Vessels SHO Programmehew ka yeePas encore d'évaluation
- Hamraki Rag April 2010 IssueDocument20 pagesHamraki Rag April 2010 IssueHamraki RagPas encore d'évaluation
- Legg Calve Perthes Disease: SynonymsDocument35 pagesLegg Calve Perthes Disease: SynonymsAsad ChaudharyPas encore d'évaluation