_
ON
ay U.S. EQUAL EMPLOYMENT OPPORTUNITY COMMISSION
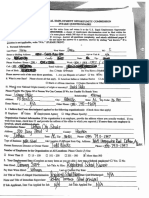
INTAKE QUESTIONNAIRE
a
Rew lease immediately complete this entire form and return it to the U.S, Equal Employment Opportunity
Commission (“EEOC”). REMEMBER, a charge of employment discrimination must be filed within the
time limits imposed by law, within 180 days or in some places within 300 days ofthe alleged discrimination. When we receive
this form, we will review ito determine EEOC coverage. Answer all questions completely, and attach additional pages if
needed to complete your responses. If you do not know the answer to a question, answer by stating “not known.” If a
‘question is not applicable, write “N/A.* (PLEASE PRINT)
1. Personal Information
Las Name:___C. Fir Name; L-QULYOL, py th
= 3 ms “AI A
County: OASHOVY sure: AL _zip:_BLFIOS
‘Suet ot Mailing Address
Sex: Male (Female Do You Have a Disability? C1 Yes\WZ°No
Please answer each of the next three questions. i. Are you Hispanic or Latino? O Yes SYNo
ii What is your Race? Please choose all hat apply. C] American Indian or Alaskan Native Cl Asian Of white
Black or African American Native Hawaiian or Other Pacific Islander
Ii, What is your National Origin ounty of origin or ancesuyy? AMNey CON,
Plesee Provide The Name OF A Person We Can Contact If We Are Unable To Reach You:
Name: SiGe HiclS Retaiontip:_ Apto OEY
adaress: PHBOY VK cig: Digbeyile—stae: PHL zip cose: 3Q310
Home Phone: (__)__ NU Other Prove: 8 7190 - HOOF _
2 Vhelive that Ywas discriminated against by te following organinstions): (Check hose that spp)
ff Employer C1 Union (1 Employment Ageney Other ene Spec) Ss
Organization Contact Information (If the organization is an employer, provide the address where you actully worked. If you
‘work from home, check here C1 and provide the address of the office to which you reported.) If more than one employer is
Gromiaton Names Stn Cu Schools
Address: BOS Dusg Secs ! was — Rous ag ——
cox DOMAN. cue ap SORDI Paw 0635 “143-15
Type of Business: ADR | Job Location if different from Org. Adares: Hoveysuctle Middle Schost.
Human Resources Direc or Owner Name: TOAG Udoees Phone: 24) 793— 347
‘Number of Employees in the Organization at All Locations: Please Check (/) One
Ol Fewer Than i5 15-100 © 101-200 201-500 More than 500
3. Your Employment Data (Complete as many items as you are able.) Are you a federal employee? 11 Yes C1 No
pare HireeFOLL QOL) sop tie arstie: SCAOOD| NUS.
Pay Rate When Hirea: ont VRCOUC rast or Current Pay Rate: QO
Job Title at Time of Alleged Discrimination: SONAL NWS, _ ate QuivDischarged: NYE
Name and Tie of immediate Supervisor: ey —TErrente,
If Job Applicant, Date You Applied for Job NY [AE Job Tite Applied For_ 0) (4
ie 9 Age Din 0 Natu Og eugion Renn O Peony Bex meas
‘hin Sheds win he soe rove) El Genvartformaton, cle wich peso Beets maton
‘my medial sory” i gene svices (pees Serves rans couing earn sng)
peo
1 you checked calor eiion of masons origin, pleme spit
{IW you checked senate information, how di the employer obulo he gens nfrmaton? WY
ter reson (a) for dieriminion Expaiy a
Nat hppane a that you ewe ws Garni? Ino Be a) of a. On
‘peta the person) who sou blew darn agate vou. Pace atach Stier ES Doe
‘Geample: 1105106 = Discharged by itt ohn Sots Toss Se
AL Date: Action: See OHadud Sass for oll
“EWS rover De
[Name and Title of Person(e) Responsible:
B. Date: ‘Action:
[Name and Titl of Person(s) Responsible
6. Why do you believe these actions were discriminatory? Please attach additonal pages if needed.
7. What reason(s) were given to you for the acts you consider discriminators? By whom? His or Her Sob Tile?
Ke .
8. Describe who was in the same or similar situation as you and how they were treated. For example, who se applica
for the same job you did, who else had the same attendance record, or who else had the same performance? Provide the
race, sex, age, national origin, religion, or disability of these individuals, if known, and if i relates to your daim of
discrimination. For example, if your complaint alleges race discrimination, provide the race of each person; i it alleges
provide the sex of each person; and so on. Use additional shests if needed.
‘sex discrimination,
(Of the persons in the same or similar situation as you, who was treated better than you?
i Description of Treatment
Race, Sex. Age, National Orig, Reliion or Dasty Jo Tie
nue, el rch er
oor a Ogee Scposi nue. n
sam Gallawxiy ent act fenea) eral, oeonMt dune
sniucs ligliler work [dod Same pay scale
2 THESE PUES alse Ga 4 neve 0 sadn Chases
like nurse Horne RN ON our work
50 ney hav, mow frre Complue Inert pape,
ee a
“ore persons in the same of snilar situation as you, who was treated were than you?
ee "Hace Sex, Age, National visio Relist or Duabily Job Tie
a Wp
WE
(Of the persons inthe same or sillr situation a¢ you, who was treated the sume a you?
‘Full Name Hace, Sex, ‘ob
Answer questions 9-12 only if you are claiming discrimination haed on disability. Ifnot, skip to question 13. Place tell
tus if you have more than one dlsabiley. Please add additional pages if needed. he
Please check all that apy: 1D Yes, Hhwve a dsb,
‘ag
Me
1D do not ave a disability now but 1 did have one
1D No disability bur the organization treats meas if am disabled
the disability chat you belive is the reason forthe adverse action taken aguint you? Docs this disability
20.
you from dolog anything? (e-., ling, seeping, breathing, walking, caring for yourself, working, et).
prevent
11, Do you wee: medical equipment or anything ele to lessen or eliminate the symptoms of your disability?
Yes No
IF Yes,” what medication, equipment or other assistance do you use?
12, Did yoo as your employer fotny changes or sistance to do your job becanse of your sity?
1f “Yes,” when did you ask? low di you ask (verbally or in writing)?
Who did you ast? (Provide fullname and jolie of person)
la
eae
How did your employer respond to your request?
‘Aes & Phone Number Wat do you believe this person willl as?
am ae
F there any witnesses to the alleged discriminatory incidents? I identify them below and tell us what
yy Ee “7
3 ‘Ell Name Job Title
14, Have yu fled a charge previwly on hs miter wit the EOC waster agaey? Yes W/o
15. Ifyou filed 2 complaint with another agency, provide the mame of agency and the date offing: _N)|O
16. ‘Have yor sought help about this situation from 2 union, an attorney, or any other source? Wifes Ol No
Prpuide pame of organization, nang of person you spe with an date of coset. Real, 3577
You would Ike ur do wi he fformation yoo ae providing o this
‘questionnaire. Ifyou woud lie 1 lea charge of jab dscriainaton, you mst 6 so ether win 180 days rom te ay yo
‘new abowt the discrimination, or within 300 day om he day you ew abou ihe discrimination if te employers Ioeated in
4a place where sae o local goverment agency enforces laws snr othe EEOC's laws. If you do nt fea charge of
‘isrimination within the tine limits, you wil lose sour rights. Ifyou would ke mare information before fling 2 charge
‘or you have concerns about EEOC's notifying the employer, ios, or employment agency about your charge, Sou ma}
wish to check Box I. Ifyou want wo flea charge, you should check Box 2.
BOX 1 O11 wart to ak wan EEOC employe before doing wiser w fle a care. Yuderand tat by checking tis box,
have not fled a charge with the EEOC. Talo understand that 1 cold lee tay tgs iT donot ea charge in te.
BOX 2 WT wan to file a charge of discrimination, and | euthorize the EEOC to look into the discrimination | described above.
Tundersand dat the EEOC must give the employer, union, or emplayment agency that Iaccue of dicrinination
information aboot the charge, including my name. Ils understand that be EEOC can only cept carps of ob
Vous aimerez peut-être aussi
- Open Meetings Law Primer RVDocument63 pagesOpen Meetings Law Primer RVRickey StokesPas encore d'évaluation
- Newsome RulingDocument3 pagesNewsome RulingRickey StokesPas encore d'évaluation
- Lee v. DHRDocument9 pagesLee v. DHRRickey StokesPas encore d'évaluation
- Grecu Memo Support SJDocument8 pagesGrecu Memo Support SJRickey StokesPas encore d'évaluation
- Plaintiff'S Response To Motion For Summary Judgment: FactsDocument7 pagesPlaintiff'S Response To Motion For Summary Judgment: FactsRickey StokesPas encore d'évaluation
- Donald Valenza ResumeDocument18 pagesDonald Valenza ResumeRickey StokesPas encore d'évaluation
- SB31 IntDocument5 pagesSB31 IntRickey StokesPas encore d'évaluation
- Grecu ComplaintDocument7 pagesGrecu ComplaintRickey StokesPas encore d'évaluation
- Supporting DocumentsDocument28 pagesSupporting DocumentsRickey StokesPas encore d'évaluation
- Food BankDocument1 pageFood BankRickey StokesPas encore d'évaluation
- Grecu Mot Summary JudgementDocument2 pagesGrecu Mot Summary JudgementRickey StokesPas encore d'évaluation
- Witness ListDocument8 pagesWitness ListRickey StokesPas encore d'évaluation
- Gov U S SenateDocument8 pagesGov U S SenateRickey StokesPas encore d'évaluation
- In The Circuit Court of Houston County, AlabamaDocument1 pageIn The Circuit Court of Houston County, AlabamaRickey StokesPas encore d'évaluation
- Del Marsh Single PageDocument1 pageDel Marsh Single PageRickey StokesPas encore d'évaluation
- Mot Dismiss 6th TimeDocument7 pagesMot Dismiss 6th TimeRickey StokesPas encore d'évaluation
- Ashford ComplaintDocument7 pagesAshford ComplaintRickey StokesPas encore d'évaluation
- Horne ComplaintDocument4 pagesHorne ComplaintRickey StokesPas encore d'évaluation
- Prosecution and Dismissal of AppealDocument2 pagesProsecution and Dismissal of AppealRickey StokesPas encore d'évaluation
- Holder ConspiracyDocument2 pagesHolder ConspiracyRickey StokesPas encore d'évaluation
- Document - Columbia Senior Citizens SARCOA Letter - Created May 01, 2017Document3 pagesDocument - Columbia Senior Citizens SARCOA Letter - Created May 01, 2017Rickey StokesPas encore d'évaluation
- Stokes Motion Dismiss PDFDocument5 pagesStokes Motion Dismiss PDFRickey StokesPas encore d'évaluation
- Driver 031717Document1 pageDriver 031717Rickey StokesPas encore d'évaluation
- WAGE Study Alabama Association of County CommissionersDocument293 pagesWAGE Study Alabama Association of County CommissionersRickey StokesPas encore d'évaluation
- State CertificationDocument3 pagesState CertificationRickey StokesPas encore d'évaluation
- In The Circuit Court of Henry County, AlabamaDocument1 pageIn The Circuit Court of Henry County, AlabamaRickey StokesPas encore d'évaluation
- Commission MeetingDocument1 pageCommission MeetingRickey StokesPas encore d'évaluation
- Dothan Response NewsomeDocument16 pagesDothan Response NewsomeRickey StokesPas encore d'évaluation
- Right To Appeal Municipal To District PDFDocument2 pagesRight To Appeal Municipal To District PDFRickey StokesPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)