Vous aimerez peut-être aussi
- Hypertension & Heart FailureDocument31 pagesHypertension & Heart FailureTj WillyPas encore d'évaluation
- HTN Treatment AlgorithmDocument1 pageHTN Treatment AlgorithmKati GrissomPas encore d'évaluation
- Management of Hypertension in DMDocument22 pagesManagement of Hypertension in DMNathania Nadia BudimanPas encore d'évaluation
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibPas encore d'évaluation
- Management of Acute Coronary Syndrome / NSTEMI: Purpose of The GuidelineDocument7 pagesManagement of Acute Coronary Syndrome / NSTEMI: Purpose of The GuidelineSahera Nurhidayah NasutionPas encore d'évaluation
- Management of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsDocument8 pagesManagement of Type 2 Diabetes Mellitus: Quick Reference Guide For Healthcare ProfessionalsAqilah SyafiqahPas encore d'évaluation
- JNC 8 PDFDocument15 pagesJNC 8 PDFcut herlindaPas encore d'évaluation
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocument56 pagesAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamPas encore d'évaluation
- Slide RTM Bioprexum PDFDocument20 pagesSlide RTM Bioprexum PDFoktaPas encore d'évaluation
- Lipid ManagementDocument2 pagesLipid ManagementMedicina FamiliarPas encore d'évaluation
- QR Management of Type 2 Diabetes Mellitus (5th Edition) PDFDocument8 pagesQR Management of Type 2 Diabetes Mellitus (5th Edition) PDFKai Xin100% (1)
- NACHC Statin Guideline Snapshot GenericDocument14 pagesNACHC Statin Guideline Snapshot GenericSaad KhanPas encore d'évaluation
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibPas encore d'évaluation
- AMH Hypertension PrintDocument4 pagesAMH Hypertension PrintMusharaf RehmanPas encore d'évaluation
- Hipertensi: Dr. Jamaluddin, M.Kes, SP - JPDocument82 pagesHipertensi: Dr. Jamaluddin, M.Kes, SP - JPRahmawati HamudiPas encore d'évaluation
- DR - Antonia Anna Lukito Slide - Webinar 18 April 2020Document34 pagesDR - Antonia Anna Lukito Slide - Webinar 18 April 2020fairuzPas encore d'évaluation
- Hypertension Guidelines PDFDocument10 pagesHypertension Guidelines PDFARAVINDAPas encore d'évaluation
- Beyond Blood Pressure Protection of Arb Focus On CandesartanDocument29 pagesBeyond Blood Pressure Protection of Arb Focus On CandesartanSuardy CiayadiPas encore d'évaluation
- Guidelines DyslipidDocument49 pagesGuidelines Dyslipidnoveldycb89Pas encore d'évaluation
- Patient's Name: Alindajao, Filoteo Diagnosis: CAD Date of Admission: Sex: 58yo Age: Male Height/WeightDocument1 pagePatient's Name: Alindajao, Filoteo Diagnosis: CAD Date of Admission: Sex: 58yo Age: Male Height/WeightButts McgeePas encore d'évaluation
- HPN in CKDDocument27 pagesHPN in CKDLeigh Picardal Caragos-MerinPas encore d'évaluation
- Habits Vs Evidence RAAS ARB Talk FinalDocument45 pagesHabits Vs Evidence RAAS ARB Talk Finalswaleh breik misfirPas encore d'évaluation
- Treatment of Hypertension: Jai Radhakrishnan, M.D. Division of NephrologyDocument34 pagesTreatment of Hypertension: Jai Radhakrishnan, M.D. Division of NephrologyAndika HPas encore d'évaluation
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocument59 pagesLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibPas encore d'évaluation
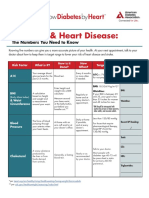
- DS 20119 KDBH Know Your Numbers PDFDocument2 pagesDS 20119 KDBH Know Your Numbers PDFjha.sofcon5941Pas encore d'évaluation
- Hypertension: Blood Pressure Classification in ChildrenDocument4 pagesHypertension: Blood Pressure Classification in ChildrenNdra NuelPas encore d'évaluation
- The Seventh Report of The Joint National Committee On Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)Document33 pagesThe Seventh Report of The Joint National Committee On Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)billi lisanuddinPas encore d'évaluation
- HypertensionDocument27 pagesHypertensionshazia kaziPas encore d'évaluation
- Prevention, Detection, Evaluation, and Management of High Blood Pressure in AdultsDocument30 pagesPrevention, Detection, Evaluation, and Management of High Blood Pressure in AdultsShazi AliPas encore d'évaluation
- The Importance of Potential Statin in High Risk PatientDocument56 pagesThe Importance of Potential Statin in High Risk PatientAidil Fittriani AyuPas encore d'évaluation
- Pocket Medicine The Massachusetts General Hospital Handbook of Internal MedicineDocument24 pagesPocket Medicine The Massachusetts General Hospital Handbook of Internal MedicineRoy Kristianto TambunanPas encore d'évaluation
- DTG - TLD Presentation For National Roll Out Training - NigeriaDocument45 pagesDTG - TLD Presentation For National Roll Out Training - NigeriaOlayinka AwofoduPas encore d'évaluation
- CPG Hypertension 2018 (Autosaved)Document55 pagesCPG Hypertension 2018 (Autosaved)Navina PurushotmananPas encore d'évaluation
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDocument18 pagesGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiPas encore d'évaluation
- HypertensionDocument18 pagesHypertensionLeoPas encore d'évaluation
- 2020 - 2022 Hypertension HighlightsDocument15 pages2020 - 2022 Hypertension HighlightsDuaa ShamiehPas encore d'évaluation
- Acs Review - Student VersionDocument3 pagesAcs Review - Student Versionapi-549451092Pas encore d'évaluation
- Virta HealthDocument18 pagesVirta Healthismail100% (1)
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919Pas encore d'évaluation
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919Pas encore d'évaluation
- Diagnosis Treatment of Resistant HypertensionDocument68 pagesDiagnosis Treatment of Resistant HypertensionJacob Alexander MarpaungPas encore d'évaluation
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095Pas encore d'évaluation
- Slide Speaker Candesartan For Hypertension in CKD PatientsDocument43 pagesSlide Speaker Candesartan For Hypertension in CKD Patientsesdras pramuditaPas encore d'évaluation
- Clinical Guidelines For Management of HTNDocument6 pagesClinical Guidelines For Management of HTNChaturangaNSenerath100% (1)
- Ilmu Penyakit Dalam: BagianDocument48 pagesIlmu Penyakit Dalam: BagianRoberto SoehartonoPas encore d'évaluation
- Hypertension GuidelinesDocument1 pageHypertension GuidelinesJuhne GioPas encore d'évaluation
- Arb in Hypertension Management: Focused On Telmisartan: Akhtar Fajar MuzakkirDocument40 pagesArb in Hypertension Management: Focused On Telmisartan: Akhtar Fajar MuzakkirFidel Martua MarpaungPas encore d'évaluation
- HIPERLIPIDEMIADocument10 pagesHIPERLIPIDEMIAMarianaPas encore d'évaluation
- L2 Hypertension in Special GroupsDocument44 pagesL2 Hypertension in Special GroupsMustaquim YusopPas encore d'évaluation
- L1 IM Hypertension (Aug2122)Document7 pagesL1 IM Hypertension (Aug2122)Maria Carmela CastilloPas encore d'évaluation
- Beyond Mountains There Are Mountains: (Haitian Proverb)Document47 pagesBeyond Mountains There Are Mountains: (Haitian Proverb)ElvisPas encore d'évaluation
- Clinical Practice Guideline For Adult Hypertension - Prevention, Screening, Counseling and ManagementDocument6 pagesClinical Practice Guideline For Adult Hypertension - Prevention, Screening, Counseling and ManagementHeppyMeiPas encore d'évaluation
- DentalManagementOfTheHypertensivePatient PDFDocument86 pagesDentalManagementOfTheHypertensivePatient PDFwalePas encore d'évaluation
- UNSW Medicine GP Management Vivas: Lawson Ung UNSW VI 2015Document41 pagesUNSW Medicine GP Management Vivas: Lawson Ung UNSW VI 2015hernandez2812Pas encore d'évaluation
- Lipids Topic DiscussionDocument10 pagesLipids Topic Discussionapi-665372449Pas encore d'évaluation
- Stroke Topic DiscussionDocument19 pagesStroke Topic Discussionapi-648714317Pas encore d'évaluation
- 2023 Measure 317 MIPSCQMDocument10 pages2023 Measure 317 MIPSCQMramshaltaf2311Pas encore d'évaluation
- I Am A Gentle: KillerDocument50 pagesI Am A Gentle: KillerMaltadillaPas encore d'évaluation
- HTN managment-JNC7Document37 pagesHTN managment-JNC7Vaibhav KaroliyaPas encore d'évaluation
- Spina BifidaDocument12 pagesSpina Bifidasalsabil aurellPas encore d'évaluation
- STD Comparison ChartDocument5 pagesSTD Comparison ChartIvy Tee100% (2)
- Cardiac Tamponade: Zhiarina Kyla M. BizDocument12 pagesCardiac Tamponade: Zhiarina Kyla M. BizMatt Joseph Cabanting100% (1)
- APGODocument49 pagesAPGOiamdonutPas encore d'évaluation
- MR Novi UapDocument25 pagesMR Novi UapAuliadi AnsharPas encore d'évaluation
- Personal History: Preterm Labor / PROMDocument7 pagesPersonal History: Preterm Labor / PROMSaber AlasmarPas encore d'évaluation
- Changing Trends in Cesarean DeliveryDocument7 pagesChanging Trends in Cesarean DeliveryEditor_IAIMPas encore d'évaluation
- CellulitisDocument15 pagesCellulitisSujatha J JayabalPas encore d'évaluation
- GDM TeachingDocument4 pagesGDM Teachingapi-272402391Pas encore d'évaluation
- McqepilipsyDocument3 pagesMcqepilipsyNguyen Anh TuanPas encore d'évaluation
- Flupentixol Injection From Injectable Drugs Guide Book - Alistair GrayDocument3 pagesFlupentixol Injection From Injectable Drugs Guide Book - Alistair Grayamin138irPas encore d'évaluation
- Enfermedad Renal CrónicaDocument41 pagesEnfermedad Renal CrónicaAndrea MedinaPas encore d'évaluation
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDocument2 pagesPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenPas encore d'évaluation
- Antibiotic ChartsDocument61 pagesAntibiotic Chartspempekplg100% (1)
- Mastering Tung AcupunctureDocument16 pagesMastering Tung AcupunctureMustafa Ali0% (1)
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaDocument10 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaAsha NopatiPas encore d'évaluation
- Dosage Chart in PaedsDocument39 pagesDosage Chart in PaedsArshad AliPas encore d'évaluation
- Myastenia GravisDocument4 pagesMyastenia Gravistimea_gheneaPas encore d'évaluation
- The Differential Diagnosis of Psoriasis Vulgaris 2376 0427 1000245Document2 pagesThe Differential Diagnosis of Psoriasis Vulgaris 2376 0427 1000245Oktavianti Prisilia SoumokilPas encore d'évaluation
- Hubungan Malnutrisi Dengan Kejadian Dismenorea Pada Remaja Putri Di Sman 1 Kampar TAHUN 2014Document8 pagesHubungan Malnutrisi Dengan Kejadian Dismenorea Pada Remaja Putri Di Sman 1 Kampar TAHUN 2014Cita Reast Wulansari83Pas encore d'évaluation
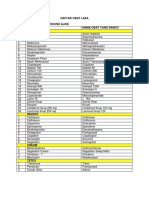
- Daftar Obat LasaDocument2 pagesDaftar Obat LasaKhalifatus SaadahPas encore d'évaluation
- ClindamycinDocument4 pagesClindamycinapi-37979410% (1)
- Daftar ObatDocument180 pagesDaftar ObatWny QaeePas encore d'évaluation
- NCLEX Random FactsDocument34 pagesNCLEX Random FactsLegnaMary100% (8)
- Stomachache and Abdominal PainDocument3 pagesStomachache and Abdominal PainHarold Sgo Jimenez GPas encore d'évaluation
- Obat BPJS SPTDocument11 pagesObat BPJS SPTpoliklinik klungkungPas encore d'évaluation
- Antimanic DrugsDocument13 pagesAntimanic DrugsGhee EvangelistaPas encore d'évaluation
- Penyakit MeniereDocument25 pagesPenyakit MeniereMuhammad Budiman Irpan BachtiarPas encore d'évaluation
- Graves BrochureDocument2 pagesGraves BrochureSussy ListiarsasihPas encore d'évaluation
- DermatologytherapyDocument642 pagesDermatologytherapyDhyna MutiarasariPas encore d'évaluation