Vous aimerez peut-être aussi
- b7d67c0f8cc2ebca94b71300f56b3e51Document42 pagesb7d67c0f8cc2ebca94b71300f56b3e51YassinSalahPas encore d'évaluation
- Svoa de 02 045Document6 pagesSvoa de 02 045YassinSalahPas encore d'évaluation
- 552ab1769123c899aed1653c45904173Document71 pages552ab1769123c899aed1653c45904173YassinSalahPas encore d'évaluation
- Resiliency in Complete DenturesDocument4 pagesResiliency in Complete DenturesYassinSalahPas encore d'évaluation
- Problems of Kennedy Class IDocument7 pagesProblems of Kennedy Class IYassinSalahPas encore d'évaluation
- Devorah SchwartzDocument2 pagesDevorah SchwartzYassinSalahPas encore d'évaluation
- Cartech Trimrite® Stainless: IdentificationDocument7 pagesCartech Trimrite® Stainless: IdentificationYassinSalahPas encore d'évaluation
- AbstractDocument1 pageAbstractYassinSalahPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Forensic Dentistry Case Book 6:: A Self-Inflicted Bite Mark A Case ReportDocument2 pagesForensic Dentistry Case Book 6:: A Self-Inflicted Bite Mark A Case ReportRizky Mega ChandraPas encore d'évaluation
- Selective Removal of Carious TissueDocument10 pagesSelective Removal of Carious TissueYovana Carolina Corimanya MoranPas encore d'évaluation
- Health Fair ProposalDocument2 pagesHealth Fair ProposalElma SintosPas encore d'évaluation
- Formato Cambra 6 Años en AdelanteDocument2 pagesFormato Cambra 6 Años en AdelanteSandra GutiérrezPas encore d'évaluation
- Cunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyDocument21 pagesCunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyMilton david Rios serratoPas encore d'évaluation
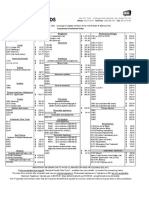
- Health and Wellness Frequently Used Dental CodesDocument1 pageHealth and Wellness Frequently Used Dental CodesNostalgia234Pas encore d'évaluation
- 999-349 Rev B Motion 3D Family BrochureDocument12 pages999-349 Rev B Motion 3D Family BrochureOrtho OrganizersPas encore d'évaluation
- Two-Point Rapid Palatal Expansion An Alternate Approach To Traditional TreatmentDocument6 pagesTwo-Point Rapid Palatal Expansion An Alternate Approach To Traditional TreatmentManena RivoltaPas encore d'évaluation
- Orthodontic Management of Patients With Cleft Lip and Palate PDFDocument6 pagesOrthodontic Management of Patients With Cleft Lip and Palate PDFcarePas encore d'évaluation
- Dipped in Holly Dana IsalyDocument29 pagesDipped in Holly Dana Isalyok cristiana100% (2)
- Complete Dentures: An Introduction: ProstheticsDocument68 pagesComplete Dentures: An Introduction: ProstheticsSahana RangarajanPas encore d'évaluation
- Revised BDS Course Regulation 2007Document101 pagesRevised BDS Course Regulation 2007VaikaviPas encore d'évaluation
- Minimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityDocument7 pagesMinimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityAnissa Citra UtamiPas encore d'évaluation
- Prostho Set 1 ADocument15 pagesProstho Set 1 ABinayak UpadhyayaPas encore d'évaluation
- Facial Nerve Ent NotesDocument8 pagesFacial Nerve Ent NotesJOSHI RAJUPas encore d'évaluation
- Artiodactyla and PerissodactylaDocument30 pagesArtiodactyla and PerissodactylaKalangiIrushikaPas encore d'évaluation
- Actividades Must/mustn TDocument3 pagesActividades Must/mustn TJosé CuencaPas encore d'évaluation
- Tweed's Philosophy - A ReviewDocument9 pagesTweed's Philosophy - A ReviewManisha PillaiPas encore d'évaluation
- Preventive ProsthodonticsDocument13 pagesPreventive Prosthodonticsbhuvanesh4668100% (1)
- Cast RstorationDocument45 pagesCast RstorationjaiminiPas encore d'évaluation
- Supportive Periodontal Therapy (SPT) For Maintaining The Dentition in Adults Treated For Periodontitis - Manresa, C - 2018 - Cochrane Library PDFDocument83 pagesSupportive Periodontal Therapy (SPT) For Maintaining The Dentition in Adults Treated For Periodontitis - Manresa, C - 2018 - Cochrane Library PDFSanjeev AthiberanPas encore d'évaluation
- Chapter Focus QuestionsDocument4 pagesChapter Focus Questionsapi-284521356Pas encore d'évaluation
- University of Medicine and Pharmacy at Ho Chi Minh City: English ClassDocument31 pagesUniversity of Medicine and Pharmacy at Ho Chi Minh City: English ClassRiin ĐặngPas encore d'évaluation
- Surgically Assisted Rapid Palatal Expansion (SARPE) A Literature ReviewDocument16 pagesSurgically Assisted Rapid Palatal Expansion (SARPE) A Literature Reviewaa bbPas encore d'évaluation
- Effect of Composite Temperature On in Vitro Intrapulpal Tempertature Rise (2006)Document6 pagesEffect of Composite Temperature On in Vitro Intrapulpal Tempertature Rise (2006)MADAPas encore d'évaluation
- List Pengadaan Barang Poli Klinik Gigi Rsud KH Mansyur 2021Document28 pagesList Pengadaan Barang Poli Klinik Gigi Rsud KH Mansyur 2021Mal FatihPas encore d'évaluation
- Centric RelationDocument50 pagesCentric RelationHarini Padmanabhan100% (1)
- School Dental Health ProgrammesDocument58 pagesSchool Dental Health Programmesindunair26Pas encore d'évaluation
- Digital Smile Design Concept PDFDocument18 pagesDigital Smile Design Concept PDFAndyRamosLopezPas encore d'évaluation
- 21st Century-Endodontics-Principles PDFDocument14 pages21st Century-Endodontics-Principles PDFLPas encore d'évaluation