Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Sketchy TrackerDocument52 pagesSketchy TrackerAzlan OmarPas encore d'évaluation
- Pharmacology For Nursing - Section I-UNit 1 - Introduction To Nursing PharmacologyCh 1&2-Dr Hanan Youssef - 40-41-1Document124 pagesPharmacology For Nursing - Section I-UNit 1 - Introduction To Nursing PharmacologyCh 1&2-Dr Hanan Youssef - 40-41-1Jnm NenPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Lewis's Medical Surgical Nursing1th Ediby Harding Test BankDocument16 pagesLewis's Medical Surgical Nursing1th Ediby Harding Test BankCarla Test BanksPas encore d'évaluation
- Respiratory System DisordersDocument115 pagesRespiratory System DisordersFaith Levi Alecha Alferez100% (1)
- Aerosol InhalotherapyDocument504 pagesAerosol Inhalotherapyjorgechung100% (1)
- Perioperative Medicine Managing Surgical Patients With Medical Problems by Chikwe, Joanna Walther, Axel Jones, PhilipDocument462 pagesPerioperative Medicine Managing Surgical Patients With Medical Problems by Chikwe, Joanna Walther, Axel Jones, PhilipIbrahim AlmohiniPas encore d'évaluation
- Pulmonary Rehabilitation and Respiratory PhysiotherapyDocument6 pagesPulmonary Rehabilitation and Respiratory PhysiotherapyHAMMYER ALROKHAMIPas encore d'évaluation
- SMLE 2019 Medicine Section 1 ReviewDocument275 pagesSMLE 2019 Medicine Section 1 ReviewPaul Asher100% (1)
- Cardiac ImagingDocument55 pagesCardiac ImagingTeuku Fadli SaniPas encore d'évaluation
- Cardiac ImagingDocument55 pagesCardiac ImagingTeuku Fadli SaniPas encore d'évaluation
- Acute Coronary Syndrome and SuicideDocument17 pagesAcute Coronary Syndrome and SuicideTeuku Fadli SaniPas encore d'évaluation
- TOEFL and Confersation Discussion ClassDocument2 pagesTOEFL and Confersation Discussion ClassRomi Mauliza FauziPas encore d'évaluation
- Cardiac Imaging PJBDocument28 pagesCardiac Imaging PJBTeuku Fadli SaniPas encore d'évaluation
- Gilman Tenth Anniversary PublicationDocument10 pagesGilman Tenth Anniversary PublicationTeuku Fadli SaniPas encore d'évaluation
- Acute Coronary Syndrome and SuicideDocument17 pagesAcute Coronary Syndrome and SuicideTeuku Fadli SaniPas encore d'évaluation
- Section 7Document2 pagesSection 7Teuku Fadli SaniPas encore d'évaluation
- Guidelines Manage Type 2 DiabetesDocument129 pagesGuidelines Manage Type 2 DiabetesTeuku Fadli SaniPas encore d'évaluation
- TOEFL and Confersation Discussion ClassDocument2 pagesTOEFL and Confersation Discussion ClassRomi Mauliza FauziPas encore d'évaluation
- Acehnese Culture(s) : Plurality and Homogeneity.: Prof. Dr. Susanne SchröterDocument31 pagesAcehnese Culture(s) : Plurality and Homogeneity.: Prof. Dr. Susanne SchröterTeuku Fadli SaniPas encore d'évaluation
- Mapping The Acehnese PastDocument40 pagesMapping The Acehnese PastTeuku Fadli SaniPas encore d'évaluation
- Funding ResearchDocument1 pageFunding ResearchTeuku Fadli SaniPas encore d'évaluation
- Poster Lomba FK UsuDocument1 pagePoster Lomba FK UsuTeuku Fadli SaniPas encore d'évaluation
- 5.sindromstevens JohnsonDocument6 pages5.sindromstevens JohnsonVia MarselinaPas encore d'évaluation
- Diabetes Mellitus: Overview and TreatmentsDocument36 pagesDiabetes Mellitus: Overview and TreatmentsTeuku Fadli SaniPas encore d'évaluation
- Presented byDocument57 pagesPresented byMB AamerPas encore d'évaluation
- Jurnal COPD Diskusi 1Document9 pagesJurnal COPD Diskusi 1Face StressorPas encore d'évaluation
- LivingwithcopdbrochureDocument3 pagesLivingwithcopdbrochureapi-676536509Pas encore d'évaluation
- Zanki Respiratory PathologyDocument15 pagesZanki Respiratory Pathologysmian08100% (1)
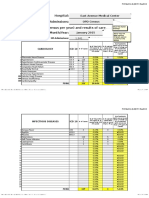
- Hospital: Admissions: Case-Load (Case Census Per Year) and Results of Care Month/YearDocument47 pagesHospital: Admissions: Case-Load (Case Census Per Year) and Results of Care Month/YearReda SoPas encore d'évaluation
- Emphysema Research ReportDocument19 pagesEmphysema Research Reportحرا مغلPas encore d'évaluation
- Diagnosing Respiratory Conditions and Diseases from SymptomsDocument9 pagesDiagnosing Respiratory Conditions and Diseases from SymptomsHaidir ArmansyahPas encore d'évaluation
- Leading Causes of MortalityDocument12 pagesLeading Causes of MortalityJayricDepalobosPas encore d'évaluation
- Cotton Dust Environments PDFDocument15 pagesCotton Dust Environments PDFRheddxymonnePas encore d'évaluation
- Warren 2009 RDSDocument13 pagesWarren 2009 RDSCIRUABCPas encore d'évaluation
- Ebook PDF The Nature of Disease Pathology For The Health Professions 2nd Edition PDFDocument41 pagesEbook PDF The Nature of Disease Pathology For The Health Professions 2nd Edition PDFherbert.critchfield195100% (38)
- Worksheet On Obstruction and AsthmaDocument14 pagesWorksheet On Obstruction and AsthmaKaye CorPas encore d'évaluation
- Republic Act No. 9163 - : Week 1 - Lesson 1 Implementing NSTP Rules and RegulationsDocument13 pagesRepublic Act No. 9163 - : Week 1 - Lesson 1 Implementing NSTP Rules and RegulationsMary Ann F. MendezPas encore d'évaluation
- Cases of Pneumonia Among Children Under Five Years Old in Bacolod City From 2019-2021Document35 pagesCases of Pneumonia Among Children Under Five Years Old in Bacolod City From 2019-2021ZeejayPas encore d'évaluation
- Care of at Risk and Sick Adult Clients With Alteration - Problems in OxygenationDocument2 pagesCare of at Risk and Sick Adult Clients With Alteration - Problems in OxygenationVinnes Ann InfantePas encore d'évaluation
- Asthma Thesis StatementDocument4 pagesAsthma Thesis Statementfjnev0hc100% (2)
- GOLD 2019 Slide SetDocument135 pagesGOLD 2019 Slide SetIhsan KPas encore d'évaluation
- IV-12 Assigmt - Module 12 Health ConditionsDocument11 pagesIV-12 Assigmt - Module 12 Health ConditionsDonnefya BravoPas encore d'évaluation
- Recurrent Pneumonia in Children: A Systematic Diagnostic ApproachDocument35 pagesRecurrent Pneumonia in Children: A Systematic Diagnostic ApproachVishal SidanaPas encore d'évaluation
- Informative SpeechDocument24 pagesInformative SpeechAnn Catherine EcitaPas encore d'évaluation
- Neonatal Respiratory Distress - A Practical Approach To Its Diagnosis and Management 2015Document17 pagesNeonatal Respiratory Distress - A Practical Approach To Its Diagnosis and Management 2015Lissey FloresPas encore d'évaluation
- ACCA Toolkit Abridged VersionDocument124 pagesACCA Toolkit Abridged VersionBianca BiaPas encore d'évaluation