Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- N2O Analgesia and AltitudeDocument4 pagesN2O Analgesia and AltitudeaksinuPas encore d'évaluation
- Extubation After AnaesthesiaDocument7 pagesExtubation After AnaesthesiaaksinuPas encore d'évaluation
- Failure To VentilateDocument2 pagesFailure To VentilateaksinuPas encore d'évaluation
- Genetic Dis & AnaesthDocument19 pagesGenetic Dis & AnaesthaksinuPas encore d'évaluation
- Fatal Drug Errors in AnaesthesiaDocument2 pagesFatal Drug Errors in AnaesthesiaaksinuPas encore d'évaluation
- Experience With A Versatile Anaesthesia MachineDocument2 pagesExperience With A Versatile Anaesthesia MachineaksinuPas encore d'évaluation
- Evaluation of Tuskmask' As An Oxygen Delivery System PDFDocument6 pagesEvaluation of Tuskmask' As An Oxygen Delivery System PDFaksinuPas encore d'évaluation
- Entrapped Epidural CatheterDocument3 pagesEntrapped Epidural CatheteraksinuPas encore d'évaluation
- Ergonomical Aspects of Anaesthetic PracticeDocument6 pagesErgonomical Aspects of Anaesthetic PracticeaksinuPas encore d'évaluation
- Error Modelling in AnaesthesiaDocument3 pagesError Modelling in AnaesthesiaaksinuPas encore d'évaluation
- Epidural Blood PatchDocument8 pagesEpidural Blood PatchaksinuPas encore d'évaluation
- Epidural Anaesthesia and ParaplegiaDocument6 pagesEpidural Anaesthesia and ParaplegiaaksinuPas encore d'évaluation
- Epinephrine During Cardiac ArrestDocument13 pagesEpinephrine During Cardiac ArrestaksinuPas encore d'évaluation
- Endocrine AnesthesiaDocument3 pagesEndocrine AnesthesiaaksinuPas encore d'évaluation
- Empowering Anesthesiologists JAnaesthClinPharmacol313291 4626976 - 011706Document2 pagesEmpowering Anesthesiologists JAnaesthClinPharmacol313291 4626976 - 011706aksinuPas encore d'évaluation
- Does Levobupivacaine Have A Benefi T Over Bupivacaine PDFDocument9 pagesDoes Levobupivacaine Have A Benefi T Over Bupivacaine PDFaksinuPas encore d'évaluation
- Effects of Changes in Intraoperative Management On Recovery From AnesthesiaDocument9 pagesEffects of Changes in Intraoperative Management On Recovery From AnesthesiaaksinuPas encore d'évaluation
- To Mix or Not To MixDocument4 pagesTo Mix or Not To MixFaizan MazharPas encore d'évaluation
- Efficacy and Safety of Intravenous Lidocaine For Postoperative Analgesia and Recovery After SurgeryDocument25 pagesEfficacy and Safety of Intravenous Lidocaine For Postoperative Analgesia and Recovery After SurgeryaksinuPas encore d'évaluation
- Early Goal-Directed Therapy Takes Another HitDocument2 pagesEarly Goal-Directed Therapy Takes Another HitaksinuPas encore d'évaluation
- EffectofNoninvasiveVentilationDeliveredbyHelmet Vs FMDocument7 pagesEffectofNoninvasiveVentilationDeliveredbyHelmet Vs FMaksinuPas encore d'évaluation
- Does Appendicitis Have To Be Treated With SurgeryDocument2 pagesDoes Appendicitis Have To Be Treated With SurgeryaksinuPas encore d'évaluation
- Critical Elements For The Pediatric Peri Op AnaesthDocument8 pagesCritical Elements For The Pediatric Peri Op AnaesthaksinuPas encore d'évaluation
- Developments in The Management of Diabetic Ketoacidosis in AdultsDocument12 pagesDevelopments in The Management of Diabetic Ketoacidosis in AdultsaksinuPas encore d'évaluation
- Depth of Insertion of Right Internal Jugular Central Venous CatheterDocument4 pagesDepth of Insertion of Right Internal Jugular Central Venous CatheteraksinuPas encore d'évaluation
- Delayed RecoveryDocument3 pagesDelayed RecoveryaksinuPas encore d'évaluation
- Complications of Regiona... A in Obstetric PracticeDocument9 pagesComplications of Regiona... A in Obstetric PracticeaksinuPas encore d'évaluation
- Concerns About Usage of Smartphones in Operating RoomDocument8 pagesConcerns About Usage of Smartphones in Operating RoomaksinuPas encore d'évaluation
- Insulina SC UciDocument18 pagesInsulina SC Ucigiseladelarosa2006Pas encore d'évaluation
- Comparison of Peripheral Nerve Stimulator Versus Usg Guided Axillary BlockDocument5 pagesComparison of Peripheral Nerve Stimulator Versus Usg Guided Axillary BlockaksinuPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hypersensitivity Rev BWDocument34 pagesHypersensitivity Rev BWGuhanPas encore d'évaluation
- 4 - Basic Food Safety and Hygiene TrainingDocument37 pages4 - Basic Food Safety and Hygiene TrainingMassi LrdPas encore d'évaluation
- CopdDocument20 pagesCopdDhanesh B MPas encore d'évaluation
- Cefuroxime Axetil MSDSDocument7 pagesCefuroxime Axetil MSDSkamelPas encore d'évaluation
- Current Management of Anaphylaxis: A FT BrownDocument12 pagesCurrent Management of Anaphylaxis: A FT BrowndoctorniravPas encore d'évaluation
- EPIPENDocument2 pagesEPIPENLana MohPas encore d'évaluation
- !! 2020 Drug Hypersensitivity ReactionsDocument12 pages!! 2020 Drug Hypersensitivity ReactionsdregleavPas encore d'évaluation
- Health7 Q4 Mod1 PreventionandControlofdiseasesanddisorders 05102021Document25 pagesHealth7 Q4 Mod1 PreventionandControlofdiseasesanddisorders 05102021Marlex Rovic ArgaoPas encore d'évaluation
- Nursing Management of Children With Bronchial AsthmaDocument17 pagesNursing Management of Children With Bronchial AsthmaalmishalnetPas encore d'évaluation
- Nursing Care Plan For Osteomyelitis: Nursing Diagnosis For Osteomyelitis and Nursing Interventions For OsteomyelitisDocument43 pagesNursing Care Plan For Osteomyelitis: Nursing Diagnosis For Osteomyelitis and Nursing Interventions For Osteomyelitisabe abdiPas encore d'évaluation
- Her Majesty's Naval Service Eligibility and Guidance Notes: WWW - Royalnavy.mod - UkDocument7 pagesHer Majesty's Naval Service Eligibility and Guidance Notes: WWW - Royalnavy.mod - UkSamuel AlexanderPas encore d'évaluation
- Journal of Oral and Maxillofacial Surgery - HealthFirstDocument333 pagesJournal of Oral and Maxillofacial Surgery - HealthFirstDodo AlvaPas encore d'évaluation
- Chapter 54 - Drugs Acting On The Upper Respiratory TractDocument13 pagesChapter 54 - Drugs Acting On The Upper Respiratory TractJonathonPas encore d'évaluation
- Charles Maytum, Rochester, MinnDocument6 pagesCharles Maytum, Rochester, Minngopal08Pas encore d'évaluation
- Lingual Tonsil Hypertrophy in Patients With Allergic RhinitisDocument6 pagesLingual Tonsil Hypertrophy in Patients With Allergic RhinitisandiniPas encore d'évaluation
- Safety Data Sheet: SupplierDocument6 pagesSafety Data Sheet: SupplierShahid BhattiPas encore d'évaluation
- Community ResourcesDocument30 pagesCommunity Resourcesapi-242881060Pas encore d'évaluation
- Nursing Process Focus: Patients Receiving Fluticasone (Flonase) Assessment Potential Nursing DiagnosesDocument2 pagesNursing Process Focus: Patients Receiving Fluticasone (Flonase) Assessment Potential Nursing DiagnosesHannah Lorraine GamayonPas encore d'évaluation
- Conjunctivitis: by PGMI Jasleen MonrealDocument77 pagesConjunctivitis: by PGMI Jasleen MonrealJade MonrealPas encore d'évaluation
- Allergic Contact by PolyethyleneDocument2 pagesAllergic Contact by PolyethyleneFreddy RojasPas encore d'évaluation
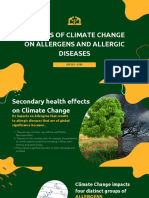
- Impacts of Climate Change On Allergens and Allergic DiseasesDocument12 pagesImpacts of Climate Change On Allergens and Allergic Diseasesmeia quiderPas encore d'évaluation
- Four Homeopathic Medicines For AsthmaDocument38 pagesFour Homeopathic Medicines For AsthmapnogrlPas encore d'évaluation
- Allergic RhinitisDocument8 pagesAllergic RhinitisJuanPas encore d'évaluation
- Antihistamines and Allergy: Katrina L RandallDocument4 pagesAntihistamines and Allergy: Katrina L RandalldhilahPas encore d'évaluation
- Health HistoryDocument1 pageHealth Historymolly_hayes_24Pas encore d'évaluation
- Chapter 16Document10 pagesChapter 16missy23pap50% (2)
- Impaired Home Maintenance in AstmaDocument2 pagesImpaired Home Maintenance in AstmaastiPas encore d'évaluation
- Anti-Asthmatic Potential of Dried Draco SpilopterusDocument6 pagesAnti-Asthmatic Potential of Dried Draco SpilopterusNxxxPas encore d'évaluation
- Bio AllergyDocument7 pagesBio AllergyShashwat YadavPas encore d'évaluation
- Food-Related Illnesses and Allergies (New)Document57 pagesFood-Related Illnesses and Allergies (New)coosa liquorsPas encore d'évaluation