Vous aimerez peut-être aussi
- JHNSNHSStudent AppDocument3 pagesJHNSNHSStudent AppAldo ChowPas encore d'évaluation
- NMTC-Application-Form-Final (1)Document5 pagesNMTC-Application-Form-Final (1)icttumainiPas encore d'évaluation
- LEAD Scholarship Application FormDocument4 pagesLEAD Scholarship Application FormMauro Era III100% (1)
- Volunteer Form SampleDocument2 pagesVolunteer Form SampleJeffrey BlissiPas encore d'évaluation
- Scholarship Application 2024 1Document3 pagesScholarship Application 2024 1Abeera KhanPas encore d'évaluation
- 20200228-2020 GESP Application Form PDFDocument2 pages20200228-2020 GESP Application Form PDFMaria MacelPas encore d'évaluation
- Scholarship ApplicationDocument2 pagesScholarship ApplicationMVRUPas encore d'évaluation
- Resident Leadership Program App Packet - Nov2018Document6 pagesResident Leadership Program App Packet - Nov2018Subhasis RoyPas encore d'évaluation
- Employment / Job Application: Page 1 of 4Document4 pagesEmployment / Job Application: Page 1 of 4api-545870588Pas encore d'évaluation
- U.S. Consulate Internship Application GuideDocument7 pagesU.S. Consulate Internship Application GuidemavitakaPas encore d'évaluation
- Course Enrolment FormDocument3 pagesCourse Enrolment FormMilos ZivkovicPas encore d'évaluation
- Undergraduate Application Form-23022022Document2 pagesUndergraduate Application Form-23022022bongisebodgePas encore d'évaluation
- Internship Registration FormDocument3 pagesInternship Registration FormihdaPas encore d'évaluation
- Municipal Scholarship ApplicationDocument2 pagesMunicipal Scholarship ApplicationRuth BolongaitaPas encore d'évaluation
- Annex A R & R Form 1 (Nomination Form)Document6 pagesAnnex A R & R Form 1 (Nomination Form)Jasmin Kerre VillarinPas encore d'évaluation
- CAS Proposal FormDocument2 pagesCAS Proposal FormCatherine Savage Wright100% (2)
- Candidate Application Form V2 23 June 2015 Neo EltariDocument4 pagesCandidate Application Form V2 23 June 2015 Neo Eltarianita nahakPas encore d'évaluation
- FSPS Program Application FormDocument1 pageFSPS Program Application FormVernadette De GuzmanPas encore d'évaluation
- Edna Gonzalez 314 E. Hutchison Dr. San Marcos TX Epg23@txstate - Edu 409-543-6404 A04869958 Computer ScienceDocument4 pagesEdna Gonzalez 314 E. Hutchison Dr. San Marcos TX Epg23@txstate - Edu 409-543-6404 A04869958 Computer ScienceEdna GonzalezPas encore d'évaluation
- Background Investigation Form: Please Fill All Information in PRINTED. If Item Is Not Applicable Put "N/A"Document5 pagesBackground Investigation Form: Please Fill All Information in PRINTED. If Item Is Not Applicable Put "N/A"jekay acay0% (1)
- Internship Registration FormDocument3 pagesInternship Registration FormMutchu TibcoPas encore d'évaluation
- Learning AgreementDocument3 pagesLearning AgreementSpaceboi.XPas encore d'évaluation
- KamoshitaDocument4 pagesKamoshitaapi-532097424Pas encore d'évaluation
- Application Form ASTON BintaroDocument3 pagesApplication Form ASTON BintaroROOMS ARTOTEL CASA CIKARANGPas encore d'évaluation
- Job ApplicationDocument4 pagesJob Applicationapi-546988246Pas encore d'évaluation
- Solon Job Application FormDocument4 pagesSolon Job Application FormBecca WicklundPas encore d'évaluation
- LANI Scholarship Application Form For College & Board or Bar Takers-rev-Oct 1.2012Document4 pagesLANI Scholarship Application Form For College & Board or Bar Takers-rev-Oct 1.2012JeaYangPas encore d'évaluation
- Student Application Packet 2012Document4 pagesStudent Application Packet 2012dawnelecePas encore d'évaluation
- Appplication FormDocument8 pagesAppplication FormDannaRoseGonzalesPas encore d'évaluation
- London Kids Admn Form - CDRDocument4 pagesLondon Kids Admn Form - CDRDeeniyat ChanserpurPas encore d'évaluation
- BGLC Scholarship Application FormDocument5 pagesBGLC Scholarship Application FormVernon WhitePas encore d'évaluation
- Form 06 Placement Proposal Form (SARAGENA).DocxDocument2 pagesForm 06 Placement Proposal Form (SARAGENA).Docx18103696Pas encore d'évaluation
- Application FormDocument6 pagesApplication FormAkshay SharmaPas encore d'évaluation
- Lease ApplicationDocument4 pagesLease ApplicationMy PG HousePas encore d'évaluation
- World Vision Application FormDocument7 pagesWorld Vision Application FormPrateek Lal60% (10)
- EDSP Application FormDocument4 pagesEDSP Application FormDave MillaresPas encore d'évaluation
- Beneficiary Identification FormDocument2 pagesBeneficiary Identification FormeugenePas encore d'évaluation
- ContohDocument4 pagesContohhrddenpasar43Pas encore d'évaluation
- AIMST University Industrial Training LogbookDocument3 pagesAIMST University Industrial Training Logbooksugaasiny shamugamPas encore d'évaluation
- Empapp 2016 BDocument5 pagesEmpapp 2016 Bapi-393899350Pas encore d'évaluation
- DAV Centenary Public School Teacher Application InstructionsDocument5 pagesDAV Centenary Public School Teacher Application InstructionsNitin SharmaPas encore d'évaluation
- Ms PM Admission FormDocument6 pagesMs PM Admission FormMuhammad Wasim AkramPas encore d'évaluation
- Oil and Gas Scholarship Application DeadlineDocument5 pagesOil and Gas Scholarship Application Deadlineee0785Pas encore d'évaluation
- The Information Given Will Be Treated in The Strictest ConfidenceDocument1 pageThe Information Given Will Be Treated in The Strictest ConfidenceGamini PereraPas encore d'évaluation
- Intake 2017-2018Document2 pagesIntake 2017-2018api-372426982Pas encore d'évaluation
- Internship Approval FormDocument1 pageInternship Approval FormmamabangoPas encore d'évaluation
- Internship Approval FormDocument1 pageInternship Approval FormmamabangoPas encore d'évaluation
- Internship Approval FormDocument1 pageInternship Approval FormmamabangoPas encore d'évaluation
- Internship Approval FormDocument1 pageInternship Approval FormmamabangoPas encore d'évaluation
- THC Information Sign-Up Form English Fillable ToolkitDocument2 pagesTHC Information Sign-Up Form English Fillable ToolkitAsmaa El-emairyPas encore d'évaluation
- Beaconhouse Academic Scholarship Application Form: Recent Passport Sized PhotographDocument2 pagesBeaconhouse Academic Scholarship Application Form: Recent Passport Sized Photographsyed qasim bukhariPas encore d'évaluation
- Personal Information Form 10Document4 pagesPersonal Information Form 10abhishek.kumarPas encore d'évaluation
- Select 58 Award Application 2015Document6 pagesSelect 58 Award Application 2015morgansearlesPas encore d'évaluation
- X-Treme Gymnastics Registration FormDocument3 pagesX-Treme Gymnastics Registration FormMichelle SantoroPas encore d'évaluation
- PinedaDocument4 pagesPinedaapi-531992035Pas encore d'évaluation
- Wipro Company Application FormDocument4 pagesWipro Company Application FormSmital Solanki100% (1)
- History Form For AdultsDocument9 pagesHistory Form For AdultsFazal HaquePas encore d'évaluation
- OJT Exit PollDocument2 pagesOJT Exit PollhaezelPas encore d'évaluation
- Indiabulls Foundation Scholarship 2019-20: Application Form For Renewal StudentsDocument3 pagesIndiabulls Foundation Scholarship 2019-20: Application Form For Renewal StudentsMajed ShaikhPas encore d'évaluation
- Lanier Sutton Ajph 2012Document10 pagesLanier Sutton Ajph 2012JennPas encore d'évaluation
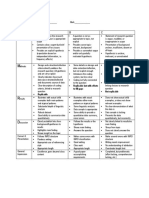
- Heading Length Content: 2018 Policy Case Competition Presentation Guidelines 1. Executive SummaryDocument2 pagesHeading Length Content: 2018 Policy Case Competition Presentation Guidelines 1. Executive SummaryJennPas encore d'évaluation
- Replicable But With Efforts To Fill Gaps Not ReplicableDocument1 pageReplicable But With Efforts To Fill Gaps Not ReplicableJennPas encore d'évaluation
- Co CurricularActivities TUEFA16Document2 pagesCo CurricularActivities TUEFA16JennPas encore d'évaluation
- Viewing GuideDocument4 pagesViewing GuideJennPas encore d'évaluation
- WCIG SupervisorForm Summer 2017Document1 pageWCIG SupervisorForm Summer 2017JennPas encore d'évaluation
- Apply for the Wasserman Center Internship Grant by February 23Document3 pagesApply for the Wasserman Center Internship Grant by February 23JennPas encore d'évaluation
- WCIG SupervisorForm Summer 2017Document1 pageWCIG SupervisorForm Summer 2017JennPas encore d'évaluation
- 2.6 Structure of DNA and RNADocument11 pages2.6 Structure of DNA and RNAJennPas encore d'évaluation
- Apply for the Wasserman Center Internship Grant by February 23Document3 pagesApply for the Wasserman Center Internship Grant by February 23JennPas encore d'évaluation
- Montgomery County Executive Hispanic Gala Educator of The Year Nomination FormDocument1 pageMontgomery County Executive Hispanic Gala Educator of The Year Nomination FormJennPas encore d'évaluation
- 2.7 DNA Replication, Transcription, and TranslationDocument25 pages2.7 DNA Replication, Transcription, and TranslationJennPas encore d'évaluation
- Estimating With Finite SumsDocument18 pagesEstimating With Finite SumsJennPas encore d'évaluation