Vous aimerez peut-être aussi
- Role of Orthodontist in Obstructive Sleep Apnea An Orthodontic ReviewDocument7 pagesRole of Orthodontist in Obstructive Sleep Apnea An Orthodontic ReviewMuhasbirPas encore d'évaluation
- Nishi Gawa 2014Document7 pagesNishi Gawa 2014MuhasbirPas encore d'évaluation
- Inflammatory Papillary Hyperplasia in A Non-Denture-Wearing Patient: A Case History ReportDocument3 pagesInflammatory Papillary Hyperplasia in A Non-Denture-Wearing Patient: A Case History ReportMuhasbirPas encore d'évaluation
- Review Article: Glue For Denture-Denture Adhesive-A ReviewDocument8 pagesReview Article: Glue For Denture-Denture Adhesive-A ReviewMuhasbirPas encore d'évaluation
- Reestablishing Esthetics With Extracted Teeth On A Mandibular Anterior Edentulous Area A Case ReportDocument3 pagesReestablishing Esthetics With Extracted Teeth On A Mandibular Anterior Edentulous Area A Case ReportMuhasbirPas encore d'évaluation
- 1 s2.0 S2352003516300296 MainDocument4 pages1 s2.0 S2352003516300296 Mainvivi AramiePas encore d'évaluation
- 10Document4 pages10MuhasbirPas encore d'évaluation
- (Ajomr)Document10 pages(Ajomr)MuhasbirPas encore d'évaluation
- 6Document11 pages6Itho SuprilPas encore d'évaluation
- Jcad 10 3 26 PDFDocument11 pagesJcad 10 3 26 PDFMuhasbirPas encore d'évaluation
- Goo Jurnal MukokelDocument4 pagesGoo Jurnal MukokelRhea Zarna IrsataniPas encore d'évaluation
- 1622 9 4 11 NitrDocument6 pages1622 9 4 11 Nitrcak_sugenkPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Guillain - Barre - SyndromeDocument18 pagesGuillain - Barre - SyndromeRAMPas encore d'évaluation
- Notes From USMLE Step 1 Goljan LecturesDocument40 pagesNotes From USMLE Step 1 Goljan Lecturesgb100% (1)
- Specimen Collection MicrobiologyDocument25 pagesSpecimen Collection MicrobiologyHartiniPas encore d'évaluation
- IFU COVID-19 Antigen Testú¿FIA)Document2 pagesIFU COVID-19 Antigen Testú¿FIA)Phyo WaiPas encore d'évaluation
- LIBERTY SQUARE: 1933-1987 THE ORIGINS AND EVOLUTION OF A PUBLIC HOUSING PROJECT by Paul S. George and Thomas K. PetersenDocument16 pagesLIBERTY SQUARE: 1933-1987 THE ORIGINS AND EVOLUTION OF A PUBLIC HOUSING PROJECT by Paul S. George and Thomas K. PetersenRandom Pixels blog100% (1)
- Cholera PresentationDocument10 pagesCholera PresentationjaniPas encore d'évaluation
- Acid Fast StainDocument3 pagesAcid Fast StainMartina MicicPas encore d'évaluation
- CPC Acute AppendicitisDocument57 pagesCPC Acute AppendicitisYS Nate100% (1)
- Cholelithiasis PDFDocument2 pagesCholelithiasis PDFVishal RamanPas encore d'évaluation
- Yellow FeverDocument4 pagesYellow FeverNader SmadiPas encore d'évaluation
- Practical Notes On Antibiotics - Emtyazology Book 2nd EditionDocument18 pagesPractical Notes On Antibiotics - Emtyazology Book 2nd EditionmajdPas encore d'évaluation
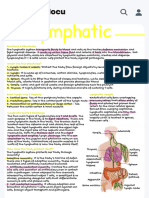
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocument1 pageHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MariePas encore d'évaluation
- Sample CollectionDocument41 pagesSample Collectionsoumen100% (1)
- Epidemiologi Penyakit TropisDocument36 pagesEpidemiologi Penyakit TropisHusein RahmatPas encore d'évaluation
- Uiip Flu Fact SheetDocument4 pagesUiip Flu Fact Sheetapi-277123092Pas encore d'évaluation
- Paediatric Chest RadiologyDocument120 pagesPaediatric Chest Radiologysunielgoel100% (6)
- HealthimpactframeworkresearchpaperyellowfeverDocument11 pagesHealthimpactframeworkresearchpaperyellowfeverapi-357823452Pas encore d'évaluation
- Colibacillosis in Calves: A Review of Literature: Bashahun, G. M. and Amina ADocument10 pagesColibacillosis in Calves: A Review of Literature: Bashahun, G. M. and Amina APrabhu KumarPas encore d'évaluation
- Covid-19 and Social DistancingDocument3 pagesCovid-19 and Social Distancinghening ciptiany pertiwyPas encore d'évaluation
- Propaganda For Tackling The 1918-19 Influenza Pandemic in Britain, With Special Reference To LondonDocument66 pagesPropaganda For Tackling The 1918-19 Influenza Pandemic in Britain, With Special Reference To LondonProtalinaPas encore d'évaluation
- Classification and General Properties of Medically Important HelminthesDocument51 pagesClassification and General Properties of Medically Important HelminthesErdem AltunPas encore d'évaluation
- Biohazardous Waste Disposal GuidelinesDocument1 pageBiohazardous Waste Disposal Guidelinesdhanaraj39Pas encore d'évaluation
- Varroosis of Honey Bees: General ProvisionsDocument4 pagesVarroosis of Honey Bees: General ProvisionsAndrew'sPas encore d'évaluation
- EQAS General InformationDocument13 pagesEQAS General Informationtanguy_chau100% (1)
- Epidemiological TriadDocument1 pageEpidemiological Triadako at ang exo100% (1)
- Necrotizing Pancreatitis - DBarilDocument25 pagesNecrotizing Pancreatitis - DBarilataner1991Pas encore d'évaluation
- A Literature Review On DengueDocument5 pagesA Literature Review On DengueFrancico XavierPas encore d'évaluation
- Gram Positive CocciDocument34 pagesGram Positive CocciMaria Cecilia Flores50% (2)
- Medication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1Document77 pagesMedication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1doodrillPas encore d'évaluation
- Evidence Over Hysteria - COVID-19 - Six Four Six Nine - MediumDocument36 pagesEvidence Over Hysteria - COVID-19 - Six Four Six Nine - MediumDorian GrayPas encore d'évaluation