Vous aimerez peut-être aussi
- Catheterisation OSCE Mark SchemeDocument2 pagesCatheterisation OSCE Mark Schememyat252Pas encore d'évaluation
- Example of Bad Answer: Press The Number of The Question To Get The AnswerDocument12 pagesExample of Bad Answer: Press The Number of The Question To Get The Answermyat252Pas encore d'évaluation
- Gallbladdercancer: Diagnosis, Surgical Management, and Adjuvant TherapiesDocument19 pagesGallbladdercancer: Diagnosis, Surgical Management, and Adjuvant Therapiesmyat252Pas encore d'évaluation
- Nervous SystemDocument62 pagesNervous Systemmyat252Pas encore d'évaluation
- Anaemia - B12 and Folate Deficiency: SummaryDocument16 pagesAnaemia - B12 and Folate Deficiency: Summarymyat252100% (1)
- Adjunctive Respiratory TherapiesDocument1 pageAdjunctive Respiratory Therapiesmyat252Pas encore d'évaluation
- Bone Marrow Transplant - Pulmonary ComplicationsDocument1 pageBone Marrow Transplant - Pulmonary Complicationsmyat252Pas encore d'évaluation
- Oncology AKT Study This Set Online atDocument1 pageOncology AKT Study This Set Online atmyat252Pas encore d'évaluation
- Opthamology AKT Study This Set Online atDocument6 pagesOpthamology AKT Study This Set Online atmyat252Pas encore d'évaluation
- Duplex Scan Kidneys: Abdo USSDocument1 pageDuplex Scan Kidneys: Abdo USSmyat252Pas encore d'évaluation
- MeningitisDocument2 pagesMeningitismyat252Pas encore d'évaluation
- CSA ABC 50 Top Tips To Pass The CSADocument25 pagesCSA ABC 50 Top Tips To Pass The CSAmyat252Pas encore d'évaluation
- Racgp GuideDocument28 pagesRacgp Guidemyat252100% (1)
- Liver Segments Explained With MnemonicDocument13 pagesLiver Segments Explained With Mnemonicmyat252100% (1)
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDocument3 pagesAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Children Types by BorlandDocument35 pagesChildren Types by BorlandHomeopathy Torrents80% (15)
- Contact Lens and Anterior Eye: Dayron F. Martínez-Pulgarín, Marcel Y. Avila, Alfonso J. Rodríguez-MoralesDocument8 pagesContact Lens and Anterior Eye: Dayron F. Martínez-Pulgarín, Marcel Y. Avila, Alfonso J. Rodríguez-MoralesAndi SilpiaPas encore d'évaluation
- Summary OphthalmologyDocument86 pagesSummary Ophthalmologymarina_shawkyPas encore d'évaluation
- Superficie Ocular ConejosDocument14 pagesSuperficie Ocular ConejosRueca HelenciyaPas encore d'évaluation
- Conjunctivitis - UpToDateDocument18 pagesConjunctivitis - UpToDateu201416371Pas encore d'évaluation
- Clinical Skills of Eye Examination: by Dr. Hajer Ahmed Ophthalmology Specialist Omar Almukhtar University 2019-2020Document40 pagesClinical Skills of Eye Examination: by Dr. Hajer Ahmed Ophthalmology Specialist Omar Almukhtar University 2019-2020Helene AlawamiPas encore d'évaluation
- Differential Diagnosis of The Swollen Red EyeDocument8 pagesDifferential Diagnosis of The Swollen Red EyeMuthia Farah AshmaPas encore d'évaluation
- Efficacy of Topical Ivermectin For The Treatment of Cutaneous and Ocular RosaceaDocument6 pagesEfficacy of Topical Ivermectin For The Treatment of Cutaneous and Ocular RosaceaAishah FarihaPas encore d'évaluation
- Symptoms & Remedies For Dry EyesDocument6 pagesSymptoms & Remedies For Dry Eyeshatime alouiPas encore d'évaluation
- Running Head: SOAP NOTE 1Document10 pagesRunning Head: SOAP NOTE 1Galatic JupiterPas encore d'évaluation
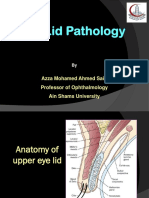
- Azza Mohamed Ahmed Said Professor of Ophthalmology Ain Shams UniversityDocument54 pagesAzza Mohamed Ahmed Said Professor of Ophthalmology Ain Shams UniversityraePas encore d'évaluation
- Ophtha LectureDocument634 pagesOphtha LectureIb YasPas encore d'évaluation
- AECP-Essentials of Ophthalmology PDFDocument235 pagesAECP-Essentials of Ophthalmology PDFsandeepPas encore d'évaluation
- After 5 Years I Found A Cure For Blepharitis and Meibomian Gland DysfunctionDocument23 pagesAfter 5 Years I Found A Cure For Blepharitis and Meibomian Gland Dysfunctionbarney_bestPas encore d'évaluation
- Do Not Copy: Diagnosis and Management of Allergic Conjunctivitis in Pediatric PatientsDocument12 pagesDo Not Copy: Diagnosis and Management of Allergic Conjunctivitis in Pediatric PatientsAngel LimPas encore d'évaluation
- Cornea PDFDocument465 pagesCornea PDFputraPas encore d'évaluation
- Blepharitis (Inflammation of The Lid Margins) : Demodex Brevis Mite Infestation)Document4 pagesBlepharitis (Inflammation of The Lid Margins) : Demodex Brevis Mite Infestation)Chad McleanPas encore d'évaluation
- Patient Blepharitis LeafletDocument2 pagesPatient Blepharitis LeafletPrincess ErickaPas encore d'évaluation
- Blepharitis An Inflammatory Condition of The EyelidsDocument4 pagesBlepharitis An Inflammatory Condition of The EyelidsTasyaPas encore d'évaluation
- BLEPHARITISDocument25 pagesBLEPHARITISSrijana MahatoPas encore d'évaluation
- Med Surg Sensory Sample PDFDocument30 pagesMed Surg Sensory Sample PDFShucipto DwiPas encore d'évaluation
- MCQ in OphthalmologyDocument107 pagesMCQ in OphthalmologyDr-Arsalan Zahid100% (2)
- BlepharitisDocument4 pagesBlepharitisJfdj DorPas encore d'évaluation
- Tear OsmolarityDocument5 pagesTear OsmolarityMaria Dominga Baylon DiazPas encore d'évaluation
- Ocular Bacterial Infections, Pathogenesis and DiagnosisDocument10 pagesOcular Bacterial Infections, Pathogenesis and DiagnosisOsmarUrielReyesAscencioPas encore d'évaluation
- MD PW 1,2 Eyelids and AnatomyDocument84 pagesMD PW 1,2 Eyelids and Anatomytaliya. shvetzPas encore d'évaluation
- Eyelash AssessmentDocument6 pagesEyelash Assessmentabee100% (2)
- Isolation and Identification of Microbial Pathogens Among Eyelash Extension Users in Imo State University, Owerri.Document7 pagesIsolation and Identification of Microbial Pathogens Among Eyelash Extension Users in Imo State University, Owerri.KIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Dr. Sadeli Masria, DR., SPMK., Ms. DMMDocument64 pagesDr. Sadeli Masria, DR., SPMK., Ms. DMMPraluki HerliawanPas encore d'évaluation
- Opthalmlogy MCQsDocument19 pagesOpthalmlogy MCQssimi y100% (2)