Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Treat Parasites by Prof Keith Scott MumbyDocument103 pagesTreat Parasites by Prof Keith Scott MumbyMunib Ahmad100% (4)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Grays Anatomy For Students 5th Edition 2023Document16 pagesGrays Anatomy For Students 5th Edition 2023AnandSreePas encore d'évaluation
- Step 2 CK PT SafetyDocument3 pagesStep 2 CK PT SafetyAhmed100% (3)
- Using Master Tung's Gallbladder Points For Diseases of The Head and NeckDocument2 pagesUsing Master Tung's Gallbladder Points For Diseases of The Head and NeckTrần Hồ Thạnh Phú100% (1)
- Nasal Polyps Grade IIIDocument2 pagesNasal Polyps Grade IIIRyan John Bito-onPas encore d'évaluation
- Chapter 15 Lung Pathology ErnieDocument20 pagesChapter 15 Lung Pathology ErnieZandra Lyn AlundayPas encore d'évaluation
- Nclex PointersDocument4 pagesNclex PointersCarl Michael de Guzman75% (12)
- CONFERENCE Direct Shear Strength Properties of Limestone-Blended PDFDocument6 pagesCONFERENCE Direct Shear Strength Properties of Limestone-Blended PDFbagus yosan setiawanPas encore d'évaluation
- Directional-Drilling To Multilateral DrillingDocument10 pagesDirectional-Drilling To Multilateral Drillingbagus yosan setiawanPas encore d'évaluation
- Paper ASP PetrofacDocument12 pagesPaper ASP Petrofacbagus yosan setiawanPas encore d'évaluation
- PB GeologyDocument116 pagesPB Geologybagus yosan setiawanPas encore d'évaluation
- Dental Risk Assessment FormDocument2 pagesDental Risk Assessment FormSamantha TacadPas encore d'évaluation
- Bihag Quiz Medicine AreaDocument5 pagesBihag Quiz Medicine AreaDan HizonPas encore d'évaluation
- Web Path AllDocument116 pagesWeb Path AllFYM0% (1)
- STM MCQDocument4 pagesSTM MCQapi-233655790Pas encore d'évaluation
- Case Presentation: Pre EclamsiaDocument66 pagesCase Presentation: Pre EclamsiaEugene Evan Endaya UyPas encore d'évaluation
- C2b - Hydatidiform Mole (H-Mole Pregnancy) ContentDocument4 pagesC2b - Hydatidiform Mole (H-Mole Pregnancy) ContentGLADYS MAY GUDELOS MEJIASPas encore d'évaluation
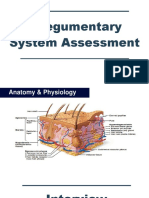
- L2 Integumentary Assessment PDFDocument46 pagesL2 Integumentary Assessment PDFElizabeth AbellaPas encore d'évaluation
- 1st PNSP Teaching Course FlyerDocument2 pages1st PNSP Teaching Course FlyerVmc PediaPas encore d'évaluation
- 2014 - SLE LectureDocument96 pages2014 - SLE LectureDon CaprettoPas encore d'évaluation
- Genesee County Health Department 2021-2022 COVID-19 School Toolkit For Schools Without Universal Mask MandatesDocument26 pagesGenesee County Health Department 2021-2022 COVID-19 School Toolkit For Schools Without Universal Mask MandatesCourtney BennettPas encore d'évaluation
- Infective Endocarditis (IE)Document76 pagesInfective Endocarditis (IE)Mahesh RathnayakePas encore d'évaluation
- Generic NameDocument7 pagesGeneric NameGia Bautista-AmbasingPas encore d'évaluation
- Strataderm BrochureDocument2 pagesStrataderm BrochureBakateriaPas encore d'évaluation
- Sample of NCP and Drug Study EPO FINAL DRUG STUDYDocument8 pagesSample of NCP and Drug Study EPO FINAL DRUG STUDYSherina BolosPas encore d'évaluation
- Lyme DisorderLLDocument14 pagesLyme DisorderLLLydia Lopz MsnrncdPas encore d'évaluation
- Pop Jordanova 67 76Document10 pagesPop Jordanova 67 76lakimkPas encore d'évaluation
- 3 - Alterations in Fluid & Electrolyte BalanceDocument62 pages3 - Alterations in Fluid & Electrolyte Balancegeng gengPas encore d'évaluation
- Rsik of ICH in Anticoagulation Primary Brain Tumor PatientDocument7 pagesRsik of ICH in Anticoagulation Primary Brain Tumor PatientFithry RahmaPas encore d'évaluation
- تجميع اسئله الاخصائين 1Document36 pagesتجميع اسئله الاخصائين 1Osama BakheetPas encore d'évaluation
- Pre Assessment Diabetes Nursing CareDocument4 pagesPre Assessment Diabetes Nursing CareHabib UllahPas encore d'évaluation
- Health and Safety Solutions Accident Investigation FormDocument2 pagesHealth and Safety Solutions Accident Investigation Formhussein aliPas encore d'évaluation
- Knee, Shin Splints, Ankle Strain, Achilles Tendinitis, Arch Pain, and Many More. All of TheDocument2 pagesKnee, Shin Splints, Ankle Strain, Achilles Tendinitis, Arch Pain, and Many More. All of TheDarko ĐorđevićPas encore d'évaluation
- Pandemic Pathogens ReportDocument17 pagesPandemic Pathogens ReportMaxwell SmartPas encore d'évaluation