Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- HP LaserJet 5P - 6P Service Manual (Proper)Document116 pagesHP LaserJet 5P - 6P Service Manual (Proper)maroudasp100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- A Dimensional Engineering Process For ShipbuildingDocument11 pagesA Dimensional Engineering Process For ShipbuildingWJccnPas encore d'évaluation
- SASMO 2020 Grade 6 + SolutionDocument24 pagesSASMO 2020 Grade 6 + SolutionBentley Leopold Halim94% (18)
- F-500 Encapsulator TechnologyDocument6 pagesF-500 Encapsulator TechnologyBdSulianoPas encore d'évaluation
- Jetty Modification - Upd 250417Document86 pagesJetty Modification - Upd 250417Deni Yudha PermanaPas encore d'évaluation
- Introduction To PragmaticsDocument119 pagesIntroduction To PragmaticsIsabella IsaBella75% (4)
- First Summative Test in Math 5 (First Quarter)Document1 pageFirst Summative Test in Math 5 (First Quarter)Marlene Tagavilla-Felipe Diculen100% (1)
- Citect V7.0 Error Codes PDFDocument13 pagesCitect V7.0 Error Codes PDFWahyu PrakosoPas encore d'évaluation
- (Nijhoff International Philosophy Series) Stanislaw Lesniewski - S. J. Surma Et Al. (Eds.) - Collected Works. 1, 2-Springer (1991)Document408 pages(Nijhoff International Philosophy Series) Stanislaw Lesniewski - S. J. Surma Et Al. (Eds.) - Collected Works. 1, 2-Springer (1991)Aldana Fontana100% (4)
- 1910 179bookletDocument12 pages1910 179bookletRichard DeNijsPas encore d'évaluation
- American Journal of Sociology Volume 46 Issue 3 1940 (Doi 10.2307/2769572) C. Wright Mills - Methodological Consequences of The Sociology of KnowledgeDocument16 pagesAmerican Journal of Sociology Volume 46 Issue 3 1940 (Doi 10.2307/2769572) C. Wright Mills - Methodological Consequences of The Sociology of KnowledgeBobi BadarevskiPas encore d'évaluation
- UDP Control and Monitoring With PIC Microcontroller - StudentCompanion PDFDocument14 pagesUDP Control and Monitoring With PIC Microcontroller - StudentCompanion PDFVport PortPas encore d'évaluation
- The Pythagorean Spiral ProjectDocument2 pagesThe Pythagorean Spiral Projectapi-316478863Pas encore d'évaluation
- Grade 6 MathDocument12 pagesGrade 6 Mathapi-264682510Pas encore d'évaluation
- TCL 55P607 CNET Review Calibration ResultsDocument3 pagesTCL 55P607 CNET Review Calibration ResultsDavid KatzmaierPas encore d'évaluation
- H-I SUPER-DEHYDRATION WITH GLYCOLSDocument15 pagesH-I SUPER-DEHYDRATION WITH GLYCOLSDiego1980bPas encore d'évaluation
- External DC fuse board for Sunny Island battery invertersDocument2 pagesExternal DC fuse board for Sunny Island battery invertersrhadammantysPas encore d'évaluation
- Primary-Side Regulation PWM Power Switch General Description FeaturesDocument10 pagesPrimary-Side Regulation PWM Power Switch General Description FeaturespopoPas encore d'évaluation
- Swat Luu: User ManualDocument13 pagesSwat Luu: User ManualgjferreiraPas encore d'évaluation
- XXXXX: Important Instructions To ExaminersDocument21 pagesXXXXX: Important Instructions To ExaminersYogesh DumanePas encore d'évaluation
- IGCSE Chemistry TEST YOUR SELF CHAPTER 4Document12 pagesIGCSE Chemistry TEST YOUR SELF CHAPTER 4Nguyễn Việt Huy RoyPas encore d'évaluation
- Oracle Database - Introduction To SQL Ed 2Document5 pagesOracle Database - Introduction To SQL Ed 2Miguel Alfonso DIAZ MORRISPas encore d'évaluation
- Darktrace Csensor Release NotesDocument10 pagesDarktrace Csensor Release NotesNelson JuniorPas encore d'évaluation
- NMNR5104 Research MethodologyDocument2 pagesNMNR5104 Research MethodologynadiaPas encore d'évaluation
- HPLC CalculatorDocument13 pagesHPLC CalculatorRamy AzizPas encore d'évaluation
- 11xx12xx SMDocument44 pages11xx12xx SMfanticelliPas encore d'évaluation
- Libro de FLOTACIÓN-101-150 PDFDocument50 pagesLibro de FLOTACIÓN-101-150 PDFIsaias Viscarra HuizaPas encore d'évaluation
- Synchronised Ujt Triggering CircuitDocument2 pagesSynchronised Ujt Triggering Circuitsvinod s67% (3)
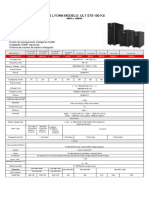
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADocument1 pageUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzPas encore d'évaluation
- Lecture 1-5 Atomic and Molecular Physics by Nek M ShaikhDocument25 pagesLecture 1-5 Atomic and Molecular Physics by Nek M Shaikh125-The Legend StarPas encore d'évaluation