Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Topic 1 Introduction To Guidance and CounsellingDocument14 pagesTopic 1 Introduction To Guidance and CounsellingNanthiniNaveesha0% (2)
- Alexander & Murphy 2000Document51 pagesAlexander & Murphy 2000amusson100% (1)
- Bodynamic Character Analysis GuideDocument22 pagesBodynamic Character Analysis GuideClara Marina Galliez100% (1)
- Peace of Mind Academic Motivation and Academic Achievement in Filipino High School StudentsDocument8 pagesPeace of Mind Academic Motivation and Academic Achievement in Filipino High School Studentsjazzy umbalPas encore d'évaluation
- Zamora Memorial College 1Document13 pagesZamora Memorial College 1darylserrano07Pas encore d'évaluation
- Model Answers CUECOR02B Work With Others: Students Assessment Marking GuideDocument2 pagesModel Answers CUECOR02B Work With Others: Students Assessment Marking Guideapi-364338283Pas encore d'évaluation
- APG Training ManualDocument94 pagesAPG Training ManualKhalid Salim100% (5)
- Defining Language, Learning and TeachingDocument65 pagesDefining Language, Learning and TeachingNatalia RóżańskaPas encore d'évaluation
- Chapter TwoDocument21 pagesChapter TwoBeka BekoPas encore d'évaluation
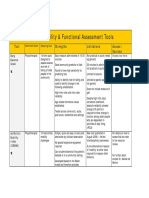
- 2013 Table 1 Mobility and Functional Assessment Tools PDFDocument4 pages2013 Table 1 Mobility and Functional Assessment Tools PDFesbat07Pas encore d'évaluation
- Teddy BearDocument6 pagesTeddy BearPâmela MuchaPas encore d'évaluation
- Learning TargetsDocument1 pageLearning TargetsCarlos Leo SantosPas encore d'évaluation
- Natural Language Processing With Deep Learning CS224N/Ling284Document62 pagesNatural Language Processing With Deep Learning CS224N/Ling284dinhmanh hoangPas encore d'évaluation
- Enhanced Job Readiness (Matthew Rowe) Case StudyDocument2 pagesEnhanced Job Readiness (Matthew Rowe) Case StudyMatthew rowePas encore d'évaluation
- How Emotional Intelligence Became A Key Leadership Skill: What To Read NextDocument12 pagesHow Emotional Intelligence Became A Key Leadership Skill: What To Read NextSintya RistriyaniPas encore d'évaluation
- Ppt-Physiological Mechanism of TasteDocument10 pagesPpt-Physiological Mechanism of TastealshmryalmwydPas encore d'évaluation
- Module 8 Neo Behaviorism Tolman and BanduraDocument8 pagesModule 8 Neo Behaviorism Tolman and Bandurashiela100% (1)
- Mental State ExaminationDocument25 pagesMental State ExaminationAyman FouadPas encore d'évaluation
- Eng 101 (Hand Outs)Document3 pagesEng 101 (Hand Outs)Mequen AlburoPas encore d'évaluation
- Music Therapy For Non - Alzheimer's Disease Dementia: A Systematic ReviewDocument9 pagesMusic Therapy For Non - Alzheimer's Disease Dementia: A Systematic ReviewMaría DiazPas encore d'évaluation
- Highly Religious Participants Recruit Areas of Social Cognition in Personal PrayerDocument9 pagesHighly Religious Participants Recruit Areas of Social Cognition in Personal PrayerIgor KhedePas encore d'évaluation
- Top-Down ApproachDocument30 pagesTop-Down ApproachDevika Vijayan100% (1)
- Insight Ciwa BPDFDocument1 pageInsight Ciwa BPDFEric McKearneyPas encore d'évaluation
- Positive Coping Strategies For College Students Under StressDocument27 pagesPositive Coping Strategies For College Students Under Stressapi-402807267Pas encore d'évaluation
- Theories of Child and Adolescent DevelopmentDocument48 pagesTheories of Child and Adolescent DevelopmentJela Marie CandaPas encore d'évaluation
- The Shallows PDFDocument6 pagesThe Shallows PDFRamona Padurean67% (3)
- Milgram's StudyDocument5 pagesMilgram's StudyMiss_M90Pas encore d'évaluation
- George Herbert MeadDocument3 pagesGeorge Herbert MeadShaina Bagacina OriolPas encore d'évaluation
- Determinants of LearningDocument22 pagesDeterminants of LearningAnthony RiggsPas encore d'évaluation
- Child Psychiatry Dr. Budi PratitiDocument16 pagesChild Psychiatry Dr. Budi PratitiRed DemonPas encore d'évaluation