Vous aimerez peut-être aussi
- Chabot Richards2014 PDFDocument10 pagesChabot Richards2014 PDFGabriel MouraPas encore d'évaluation
- 2nd Sem - Hema1 - An Overview of Clinical Laboratory HematologyDocument3 pages2nd Sem - Hema1 - An Overview of Clinical Laboratory HematologyAisle Malibiran PalerPas encore d'évaluation
- Decipher Your Labwork - CBC: Functional MedicineD'EverandDecipher Your Labwork - CBC: Functional MedicineÉvaluation : 1 sur 5 étoiles1/5 (1)
- Ijlh 1251Document6 pagesIjlh 1251Ramadhan OlongPas encore d'évaluation
- Rodaks 6th Ed. Hema Lab Midterm ReviewerDocument30 pagesRodaks 6th Ed. Hema Lab Midterm ReviewerGerald SorianoPas encore d'évaluation
- 39notes Clinical PathologyDocument9 pages39notes Clinical PathologyaymenPas encore d'évaluation
- ZP11 Xxi 63Document8 pagesZP11 Xxi 63Jai CarungayPas encore d'évaluation
- Int J Lab Hematology - 2017 - Chabot Richards - Does Morphology Matter in 2017 An Approach To Morphologic Clues inDocument8 pagesInt J Lab Hematology - 2017 - Chabot Richards - Does Morphology Matter in 2017 An Approach To Morphologic Clues inLidija MilkovskaPas encore d'évaluation
- Automated Counters3Document14 pagesAutomated Counters3Jacky SharmaPas encore d'évaluation
- Morfologi PlateletDocument24 pagesMorfologi PlateletEllya Latifah IlyasPas encore d'évaluation
- Laboratorio, Manual, Revisión de SangreDocument12 pagesLaboratorio, Manual, Revisión de SangreGaby Gómez100% (1)
- Complete Blood Cell Count and Peripheral Blood Film, Its Significant in Laboratory Medicine: A Review StudyDocument24 pagesComplete Blood Cell Count and Peripheral Blood Film, Its Significant in Laboratory Medicine: A Review StudyanggaririnPas encore d'évaluation
- 1 Hematology TestDocument48 pages1 Hematology TestAhmed YassinPas encore d'évaluation
- Morphology of HematologyDocument11 pagesMorphology of HematologyChabPas encore d'évaluation
- 05 - Peripheral Blood Smear ExaminationDocument40 pages05 - Peripheral Blood Smear Examinationaustin_doc2rPas encore d'évaluation
- Wahed2020 PDFDocument11 pagesWahed2020 PDFChaira Alkanzi DjeniPas encore d'évaluation
- CBCDocument15 pagesCBCUlicer CruzPas encore d'évaluation
- Haematology 2 ManualDocument26 pagesHaematology 2 Manualhayamitib11Pas encore d'évaluation
- 3 s2.0 B9780702066962000230 MainDocument14 pages3 s2.0 B9780702066962000230 MainKate ClarksonPas encore d'évaluation
- Anemia, Tic, DLC MbbsDocument50 pagesAnemia, Tic, DLC Mbbssharads221004Pas encore d'évaluation
- 4-Morphology Based Detection of Abnormal Red Blood Cells in Peripheral Blood Smear ImagesDocument2 pages4-Morphology Based Detection of Abnormal Red Blood Cells in Peripheral Blood Smear ImagesAli M. RiyathPas encore d'évaluation
- 04.28 Hematology PPT NotesDocument6 pages04.28 Hematology PPT Notesmlttechnologist9Pas encore d'évaluation
- SysmexDocument113 pagesSysmexARIF AHAMMED P100% (1)
- ClassificationDocument16 pagesClassificationpieterinpretoria391Pas encore d'évaluation
- Presentation (5) 2Document43 pagesPresentation (5) 2kolusam beveePas encore d'évaluation
- Answers - Haematological Malignancies Digital Images QuizDocument4 pagesAnswers - Haematological Malignancies Digital Images Quizcande casanasPas encore d'évaluation
- CP Exer 2 Examination of Peripheral Blood Smear Diff CountDocument2 pagesCP Exer 2 Examination of Peripheral Blood Smear Diff CountClyde HinloPas encore d'évaluation
- Complete Blood Count: Abdellatif Aly MohamedDocument81 pagesComplete Blood Count: Abdellatif Aly MohamedGroup 11Pas encore d'évaluation
- Understanding Blood Cell Counts: Fact SheetDocument5 pagesUnderstanding Blood Cell Counts: Fact SheetRuchira BhattacharyyaPas encore d'évaluation
- Casos Clinicos de Hematopatología IiDocument5 pagesCasos Clinicos de Hematopatología IiRicardo LaraPas encore d'évaluation
- Flowcytometryin Diagnosis, Prognostication, Andmonitoringofmultiple MyelomaandrelateddisordersDocument13 pagesFlowcytometryin Diagnosis, Prognostication, Andmonitoringofmultiple MyelomaandrelateddisordersmatanhibPas encore d'évaluation
- iMD - Uptodate - Evaluation of The Peripheral Blood SmearDocument13 pagesiMD - Uptodate - Evaluation of The Peripheral Blood Smearmohsenmaa78Pas encore d'évaluation
- Nucleated Rbcs-Significance in The Peripheral Blood Film: H He em Ma at To Ol Lo Og Gy YDocument7 pagesNucleated Rbcs-Significance in The Peripheral Blood Film: H He em Ma at To Ol Lo Og Gy YFede0Pas encore d'évaluation
- Pathological Processes and Reactive Changes in Leucocyte System Feghiu I., Tacu L.Document13 pagesPathological Processes and Reactive Changes in Leucocyte System Feghiu I., Tacu L.LunguVictoriaPas encore d'évaluation
- Heme-Onc Anki QDocument41 pagesHeme-Onc Anki Qjhk0428Pas encore d'évaluation
- Presentation On Full Blood Count by Group EightDocument15 pagesPresentation On Full Blood Count by Group Eightmaxwell amponsahPas encore d'évaluation
- (Hema Manucript) Myelophthisic Anemia FINALCMPDocument6 pages(Hema Manucript) Myelophthisic Anemia FINALCMPJohney Doe100% (1)
- Presentation On Full Blood Count by Group EightDocument15 pagesPresentation On Full Blood Count by Group Eightmaxwell amponsahPas encore d'évaluation
- Educational Commentary - A Case of Infection With A Plasmodium SpeciesDocument5 pagesEducational Commentary - A Case of Infection With A Plasmodium SpeciesReman A. AlingasaPas encore d'évaluation
- Determining The Cause: AnemiaDocument9 pagesDetermining The Cause: AnemiaSelina SubiasPas encore d'évaluation
- Sun 1996Document7 pagesSun 1996Araceli Enríquez OvandoPas encore d'évaluation
- Complete Blood Count: 1 Medical UsesDocument5 pagesComplete Blood Count: 1 Medical UsestharakaPas encore d'évaluation
- Piis0025619611615681 PDFDocument14 pagesPiis0025619611615681 PDFMaryJoy Dela CruzPas encore d'évaluation
- Atlas Hematologie CropDocument268 pagesAtlas Hematologie Cropelena31popescu100% (1)
- Case StudyDocument21 pagesCase StudyLuige AvilaPas encore d'évaluation
- Module 2 Blood and Bloostain Analysis Forensic 3Document29 pagesModule 2 Blood and Bloostain Analysis Forensic 3nikke requePas encore d'évaluation
- Hemoglobin Protein: Physical Exam HistoryDocument3 pagesHemoglobin Protein: Physical Exam HistoryAmit MartinPas encore d'évaluation
- Blood Cell MorphologyDocument5 pagesBlood Cell MorphologyKIPRUTO DENNISPas encore d'évaluation
- Lab 5 Aniphy Blood Count PDFDocument6 pagesLab 5 Aniphy Blood Count PDFNao AdunaPas encore d'évaluation
- White Blood Cells Red Blood Cells Platelets: Complete Blood Count (CBC)Document11 pagesWhite Blood Cells Red Blood Cells Platelets: Complete Blood Count (CBC)bsonPas encore d'évaluation
- Interpretasi Darah RutinDocument22 pagesInterpretasi Darah Rutinboy jendri huluPas encore d'évaluation
- Complete Blood Count: at A GlanceDocument6 pagesComplete Blood Count: at A Glancecsy123Pas encore d'évaluation
- Investigation Methods in HematologyDocument32 pagesInvestigation Methods in HematologyCarmen DuranPas encore d'évaluation
- Interferences in Platelet: CountingDocument5 pagesInterferences in Platelet: CountingIberisPas encore d'évaluation
- Complete Blood Count: What Is Being Tested?Document3 pagesComplete Blood Count: What Is Being Tested?shehnilaPas encore d'évaluation
- Chronic Myeloid Leukemia (CML) Is A Form of Leukemia CharacterizedDocument4 pagesChronic Myeloid Leukemia (CML) Is A Form of Leukemia CharacterizedbassamhematolPas encore d'évaluation
- Hematuria Science Direct 2023Document10 pagesHematuria Science Direct 2023fernanda garnicaPas encore d'évaluation
- Lab Result in EnglishDocument3 pagesLab Result in EnglishirdinamarchsyaPas encore d'évaluation
- 2021 Course Outline Operations Management Tutorial MTM C10Document5 pages2021 Course Outline Operations Management Tutorial MTM C10irdinamarchsyaPas encore d'évaluation
- Pre Training Discussion - BD FACSLyricDocument48 pagesPre Training Discussion - BD FACSLyricirdinamarchsyaPas encore d'évaluation
- The Challenges and Benefit of Internal Auditing PDFDocument27 pagesThe Challenges and Benefit of Internal Auditing PDFirdinamarchsyaPas encore d'évaluation
- Manufacture of QCDocument19 pagesManufacture of QCirdinamarchsyaPas encore d'évaluation
- Terms of ReferenceDocument3 pagesTerms of ReferenceirdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument22 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- 01 - Current Draft WHO-CDC Biosafety RecommendationsDocument32 pages01 - Current Draft WHO-CDC Biosafety RecommendationsitsruriPas encore d'évaluation
- Physicians Statement 0-2Document1 pagePhysicians Statement 0-2irdinamarchsyaPas encore d'évaluation
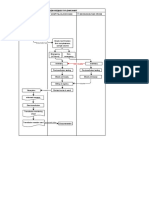
- Blood Request FlowchartDocument1 pageBlood Request FlowchartirdinamarchsyaPas encore d'évaluation
- TAT For Issuing Blood Products in EmergencyDocument4 pagesTAT For Issuing Blood Products in Emergencyirdinamarchsya100% (1)
- Antibiotik Yg Ada D RSKDDocument1 pageAntibiotik Yg Ada D RSKDirdinamarchsyaPas encore d'évaluation
- Uji Validasi Metode Tes Alat Hematologi Sysmex Xnl350Document1 pageUji Validasi Metode Tes Alat Hematologi Sysmex Xnl350irdinamarchsyaPas encore d'évaluation
- Blood Transfusion: Teoman SOYSAL Prof. MDDocument38 pagesBlood Transfusion: Teoman SOYSAL Prof. MDirdinamarchsyaPas encore d'évaluation
- Myeloproliferative Disorders by T1kaDocument48 pagesMyeloproliferative Disorders by T1kairdinamarchsyaPas encore d'évaluation
- Prinsip Kerja MGITDocument6 pagesPrinsip Kerja MGITirdinamarchsyaPas encore d'évaluation
- Use of IGRA For Diagnosis of TB PleurisyDocument7 pagesUse of IGRA For Diagnosis of TB PleurisyirdinamarchsyaPas encore d'évaluation
- Establishment of Reference Ranges For SPE in The Pediatric Population - A. FogliDocument1 pageEstablishment of Reference Ranges For SPE in The Pediatric Population - A. FogliirdinamarchsyaPas encore d'évaluation
- Neonatal Fungal InfectionDocument4 pagesNeonatal Fungal InfectionirdinamarchsyaPas encore d'évaluation
- CellDocument15 pagesCellprakash kushwahaPas encore d'évaluation
- Cell (Lesson Plan)Document4 pagesCell (Lesson Plan)aiza.coltamaiPas encore d'évaluation
- Blood Practice TestDocument13 pagesBlood Practice Testching chongPas encore d'évaluation
- 1st Midterm Biochem Evaluation Exam 2Document2 pages1st Midterm Biochem Evaluation Exam 2MaryPas encore d'évaluation
- Geriatric Nursing Theories of AgingDocument8 pagesGeriatric Nursing Theories of AgingAi RouPas encore d'évaluation
- Vacuole FunctionDocument8 pagesVacuole Functionkbansal981Pas encore d'évaluation
- Pengaruh Suhu Terhadap Kerja EnzimDocument6 pagesPengaruh Suhu Terhadap Kerja EnzimAlfrilin PadjaoPas encore d'évaluation
- Carbohydrate Metabolism BioChem Lec Finals2x1 FormatDocument3 pagesCarbohydrate Metabolism BioChem Lec Finals2x1 FormatSheene ImblarinagPas encore d'évaluation
- Full Download Genetics Essentials Concepts and Connections 3rd Edition Pierce Test Bank PDF Full ChapterDocument36 pagesFull Download Genetics Essentials Concepts and Connections 3rd Edition Pierce Test Bank PDF Full Chapternuggetessayistypcu100% (18)
- Cells and Organelles - The Microscope in Cell Study (Light and Electron Microscope)Document3 pagesCells and Organelles - The Microscope in Cell Study (Light and Electron Microscope)Robert WalusimbiPas encore d'évaluation
- Dwnload Full Method and Practice in Biological Anthropology 1st Edition Hens Solutions Manual PDFDocument36 pagesDwnload Full Method and Practice in Biological Anthropology 1st Edition Hens Solutions Manual PDFtaylorloganptglt100% (9)
- Dot Point IB Biology - AHL - Kerri Humphreys - Science 2010 PDFDocument50 pagesDot Point IB Biology - AHL - Kerri Humphreys - Science 2010 PDFJulio Cèsar Torres Hernández100% (1)
- Oliveira Magalhaes Marco A 201411 MSC Thesis PDFDocument83 pagesOliveira Magalhaes Marco A 201411 MSC Thesis PDFMahmoud AlshahatPas encore d'évaluation
- Q1 GenBio1 SLKWeek3 EditDocument20 pagesQ1 GenBio1 SLKWeek3 EditInele Ellia AgRePas encore d'évaluation
- Golgi Apparatus - WikipediaDocument17 pagesGolgi Apparatus - WikipediaPrakashananda ThakurPas encore d'évaluation
- Host Reactions To BiomaterialsDocument40 pagesHost Reactions To BiomaterialsSidekkPas encore d'évaluation
- Aquatic Animal Nutrition A Mechanistic Perspective From Individuals To GenerationsDocument490 pagesAquatic Animal Nutrition A Mechanistic Perspective From Individuals To GenerationsOnur DemirelPas encore d'évaluation
- WEEK 3 LAB EXERCISE - Cell Structures and Functions - UY-OCODocument4 pagesWEEK 3 LAB EXERCISE - Cell Structures and Functions - UY-OCOBianca LouisePas encore d'évaluation
- Krok Book PDFDocument1 282 pagesKrok Book PDFAnasse Douma100% (1)
- 9700 s11 QP 41Document28 pages9700 s11 QP 41Ahmed Kaleem Khan NiaziPas encore d'évaluation
- DNA Translation Written ReportDocument5 pagesDNA Translation Written ReportHerlene SeePas encore d'évaluation
- DNA Genes and ChromosomeDocument4 pagesDNA Genes and ChromosomeRommel BauzaPas encore d'évaluation
- Cell Parts and Functions 2Document3 pagesCell Parts and Functions 2Arshelyn Donna NovenoPas encore d'évaluation
- Result Lab Report 3Document6 pagesResult Lab Report 3Nurl AinaPas encore d'évaluation
- Lipid Transport and StorageDocument34 pagesLipid Transport and StorageGuru Kiran C KPas encore d'évaluation
- CHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate PathwayDocument12 pagesCHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate Pathway楊畯凱Pas encore d'évaluation
- Organelles Cheat SheetDocument8 pagesOrganelles Cheat Sheetapi-55809756Pas encore d'évaluation
- Quiz 3 Protein TargetingDocument6 pagesQuiz 3 Protein TargetingJeevikaGoyalPas encore d'évaluation
- Pathology Solved Papers 2015Document35 pagesPathology Solved Papers 2015Lakshmi Venkataraman100% (3)
- MICRO611Exam1 - 2014: Your Name: Your ID: # of QuestionsDocument33 pagesMICRO611Exam1 - 2014: Your Name: Your ID: # of QuestionsJacob MercierPas encore d'évaluation
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)D'EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Évaluation : 3 sur 5 étoiles3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 4 sur 5 étoiles4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisD'EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisÉvaluation : 5 sur 5 étoiles5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainD'EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainÉvaluation : 4 sur 5 étoiles4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeD'EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedÉvaluation : 4 sur 5 étoiles4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (60)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesD'EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesÉvaluation : 4.5 sur 5 étoiles4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (45)