Vous aimerez peut-être aussi
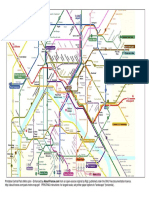
- Printable Central Paris Metro Plan - Enhanced byDocument2 pagesPrintable Central Paris Metro Plan - Enhanced byRoisinPas encore d'évaluation
- Schizophrenia Concept MapDocument1 pageSchizophrenia Concept MapGabrielle Franklin86% (7)
- Mental Health Benefits of Physical ActivityDocument8 pagesMental Health Benefits of Physical Activityarlenebraganza82Pas encore d'évaluation
- PRO Post Natal AssessmentDocument9 pagesPRO Post Natal AssessmentMali KanuPas encore d'évaluation
- Hyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDocument49 pagesHyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDonna LabaniegoPas encore d'évaluation
- SRS PostOp Care (Add Pic)Document24 pagesSRS PostOp Care (Add Pic)m1au123100% (3)
- Psychobiology and Molecular Genetics of ResilienceDocument23 pagesPsychobiology and Molecular Genetics of Resiliencemelpomena81Pas encore d'évaluation
- Article Abt HypertensionDocument8 pagesArticle Abt HypertensionG HarshythaPas encore d'évaluation
- Healthy Body, Healthy Mind?: The Psychologist January 2002Document3 pagesHealthy Body, Healthy Mind?: The Psychologist January 2002ka waiiPas encore d'évaluation
- Acm 2009 0044Document10 pagesAcm 2009 0044VaisnavaPas encore d'évaluation
- Word YogaDocument10 pagesWord YogaEry WidiantaraPas encore d'évaluation
- Bernstein McNally 2018 Behaviour Research and TherapyDocument8 pagesBernstein McNally 2018 Behaviour Research and TherapyIordache LarisaPas encore d'évaluation
- Zhang 2021Document8 pagesZhang 2021iovanelena235Pas encore d'évaluation
- SmithDocument14 pagesSmithtalliaPas encore d'évaluation
- Perceptual Insensitivity To The Modulation of InteDocument15 pagesPerceptual Insensitivity To The Modulation of IntePeter HolzerPas encore d'évaluation
- Physical Activity For Cognitive and Mental Health in Youth: A Systematic Review of MechanismsDocument15 pagesPhysical Activity For Cognitive and Mental Health in Youth: A Systematic Review of MechanismsKiki SyamPas encore d'évaluation
- Journal of Science and Medicine in SportDocument6 pagesJournal of Science and Medicine in SportTomás Delgado BlasPas encore d'évaluation
- BisbasDocument16 pagesBisbas心理谷Pas encore d'évaluation
- Actvidad Fisica y CongnicionDocument7 pagesActvidad Fisica y CongnicionluvinuosPas encore d'évaluation
- Physical Activity, Exercise, and Mental DisordersDocument8 pagesPhysical Activity, Exercise, and Mental DisordersHargo PsyPas encore d'évaluation
- Journal of Behavior Therapy and Experimental PsychiatryDocument8 pagesJournal of Behavior Therapy and Experimental PsychiatryAndré LuizPas encore d'évaluation
- Sueño y AerobicDocument10 pagesSueño y Aerobicmarcos_casasPas encore d'évaluation
- 1 s2.0 S1807593222032173 MainDocument10 pages1 s2.0 S1807593222032173 MainAyisha JaPas encore d'évaluation
- Psychology of Sport & Exercise: SciencedirectDocument10 pagesPsychology of Sport & Exercise: SciencedirectGianmarco BenottiPas encore d'évaluation
- Psych 110 - Final Empirical Paper - The Relationship Between Stress Levels and Weekly Exercise FrequencyDocument14 pagesPsych 110 - Final Empirical Paper - The Relationship Between Stress Levels and Weekly Exercise Frequencykirbysiao136Pas encore d'évaluation
- Brief, Daily Meditation Enhances Attention, Memory, Mood, and Emotional Regulation in Non-Experienced Meditators - Wendy SuzukiDocument13 pagesBrief, Daily Meditation Enhances Attention, Memory, Mood, and Emotional Regulation in Non-Experienced Meditators - Wendy Suzukiphilip.agen.businessPas encore d'évaluation
- Nihms 9803Document16 pagesNihms 9803api-291907176Pas encore d'évaluation
- YogaDocument19 pagesYogaemanuelle rodriguesPas encore d'évaluation
- Final Literature ReviewDocument6 pagesFinal Literature Reviewapi-625333741Pas encore d'évaluation
- Group 4 (Faith Dyan Arbues BPED 2A)Document9 pagesGroup 4 (Faith Dyan Arbues BPED 2A)Faith Dyan E. ArbuesPas encore d'évaluation
- Symposium: Psychophysical Bases of Perceived ExertionDocument5 pagesSymposium: Psychophysical Bases of Perceived ExertionLuis Felipe Huesca OcampoPas encore d'évaluation
- 90 10.5923.j.ijpbs.20170704.04Document12 pages90 10.5923.j.ijpbs.20170704.04Sanja Tatalovic VorkapicPas encore d'évaluation
- Actividad Fisica y Salud MentalDocument12 pagesActividad Fisica y Salud MentalDili SotoPas encore d'évaluation
- Physical Healing As A Function of Perceived Time: Peter Aungle & Ellen LangerDocument9 pagesPhysical Healing As A Function of Perceived Time: Peter Aungle & Ellen Langertincho1980Pas encore d'évaluation
- 19 Duncan2016Document7 pages19 Duncan2016Sergio Machado NeurocientistaPas encore d'évaluation
- Respiração StressDocument17 pagesRespiração StressRodrigo SantosPas encore d'évaluation
- Physical Activity Correlates Among People With Psychosis Data From 47Document6 pagesPhysical Activity Correlates Among People With Psychosis Data From 47AMIGOMEZPas encore d'évaluation
- Impact of Stress On Physical and Mental Health of An IndividualDocument7 pagesImpact of Stress On Physical and Mental Health of An IndividualNik 19Pas encore d'évaluation
- Cortical Activation Abnormalities in Bipolar and Schizophrenia Patients in A Combined Oddball-Incongruence ParadigmDocument13 pagesCortical Activation Abnormalities in Bipolar and Schizophrenia Patients in A Combined Oddball-Incongruence ParadigmSemma LopesPas encore d'évaluation
- Edinburgh Research Explorer: Physical Activity For Cognitive and Mental Health in YouthDocument28 pagesEdinburgh Research Explorer: Physical Activity For Cognitive and Mental Health in Youthlauracastillolopez2000Pas encore d'évaluation
- Exercise Enhances Creativity Independent of MoodDocument7 pagesExercise Enhances Creativity Independent of MoodLinh NguyenPas encore d'évaluation
- Artículo 3Document7 pagesArtículo 3Natalia PanchueloPas encore d'évaluation
- Exercise and The Prevention of Depression: Results of The HUNT Cohort StudyDocument9 pagesExercise and The Prevention of Depression: Results of The HUNT Cohort StudyLydia AmaliaPas encore d'évaluation
- Brjsmed00003 0076Document6 pagesBrjsmed00003 0076fnf102030Pas encore d'évaluation
- Alterations in Brain and Immune Function Produced by Mindfulness MeditationDocument8 pagesAlterations in Brain and Immune Function Produced by Mindfulness MeditationJulio LinaresPas encore d'évaluation
- HealthcareDocument10 pagesHealthcareAndrade GuiPas encore d'évaluation
- Neural Correlates of Dispositional Mindfulness During Affect Labeling-560.FullDocument6 pagesNeural Correlates of Dispositional Mindfulness During Affect Labeling-560.FullZenPas encore d'évaluation
- Rou Saud 2007Document11 pagesRou Saud 2007healliz36912Pas encore d'évaluation
- 2018 Cognitive Control Training For Emotion-Related Impulsivity.009Document10 pages2018 Cognitive Control Training For Emotion-Related Impulsivity.009Giovannino FasciasalePas encore d'évaluation
- Klompstra 2018 Self Efficacy Mediates The RelaDocument6 pagesKlompstra 2018 Self Efficacy Mediates The RelaJonathanPas encore d'évaluation
- Effects of Stretching On Menopausal and Depressive Symptoms in Middle-Aged Women: A Randomized Controlled TrialDocument6 pagesEffects of Stretching On Menopausal and Depressive Symptoms in Middle-Aged Women: A Randomized Controlled TrialGorkaBuesaPas encore d'évaluation
- Brainsci 14 00084Document14 pagesBrainsci 14 00084phybeatworkPas encore d'évaluation
- Poorer Positive Affect in Response To Self-Paced Exercise Among The ObeseDocument35 pagesPoorer Positive Affect in Response To Self-Paced Exercise Among The ObeseDouglas MarinPas encore d'évaluation
- Feature: Biofeedback and Expressive Writing: Emotional Disclosure and Its Effects On HealthDocument6 pagesFeature: Biofeedback and Expressive Writing: Emotional Disclosure and Its Effects On Healthapi-193771047Pas encore d'évaluation
- Is Paid Period Leave Justified in Working Women: A Crossectional StudyDocument5 pagesIs Paid Period Leave Justified in Working Women: A Crossectional StudyEiman Khowaja (22GJKB-CLSTEC)Pas encore d'évaluation
- Gaab Et Al., 2005Document12 pagesGaab Et Al., 2005Paulina Arjona JzPas encore d'évaluation
- Journal Pcbi 1008484Document31 pagesJournal Pcbi 1008484thinh_41Pas encore d'évaluation
- Emotion, Stress, and Cardiovascular Response: An Experimental Test of Models of Positive and Negative AffectDocument6 pagesEmotion, Stress, and Cardiovascular Response: An Experimental Test of Models of Positive and Negative AffectEva NovitaPas encore d'évaluation
- Be Smart, Exercise Your Heart - Exercise Effects On Brain and CognitionDocument8 pagesBe Smart, Exercise Your Heart - Exercise Effects On Brain and CognitionMakanudo.Pas encore d'évaluation
- Achim 2012 PR (MTZ-FEP)Document7 pagesAchim 2012 PR (MTZ-FEP)richard LemieuxPas encore d'évaluation
- A Wrinkle in Measuring Time Use For Cognitive Health How Should We Measure Physical Activity SedentaryDocument18 pagesA Wrinkle in Measuring Time Use For Cognitive Health How Should We Measure Physical Activity Sedentarymededep273Pas encore d'évaluation
- Mandal, Arya & Pandey, 2012Document10 pagesMandal, Arya & Pandey, 2012Satchit Prasun MandalPas encore d'évaluation
- Biological Correlates of Reiki Touch HealingDocument7 pagesBiological Correlates of Reiki Touch HealinglapastorinhaPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptFrontiersPas encore d'évaluation
- No Fry Fried RiceDocument1 pageNo Fry Fried RiceRoisinPas encore d'évaluation
- Homemade Chicken Nuggets: IngredientsDocument2 pagesHomemade Chicken Nuggets: IngredientsRoisinPas encore d'évaluation
- Watermelon and Feta SaladDocument1 pageWatermelon and Feta SaladRoisinPas encore d'évaluation
- Versailles Palace: ParisDocument2 pagesVersailles Palace: ParisRoisinPas encore d'évaluation
- Roasted Spring Vegetables - Bless This MessDocument2 pagesRoasted Spring Vegetables - Bless This MessRoisinPas encore d'évaluation
- Mexican Restaurant-Style Cauliflower RiceDocument2 pagesMexican Restaurant-Style Cauliflower RiceRoisinPas encore d'évaluation
- Cardiovascular Circuit TrainingDocument1 pageCardiovascular Circuit TrainingRoisinPas encore d'évaluation
- Curried Potato PastiesDocument2 pagesCurried Potato PastiesRoisinPas encore d'évaluation
- Banana Muffins: IngredientsDocument1 pageBanana Muffins: IngredientsRoisinPas encore d'évaluation
- Belfast PlanoDocument2 pagesBelfast PlanoCaro DiazPas encore d'évaluation
- 1 Normal Press-Ups 2 Crunchies 3 Squat Thrusts 4 Bench Dips 5 Normal Sit-Ups 6 Jump Squats 7 Decline Press-Ups 8 Half Sit-Ups 9 BurpeesDocument2 pages1 Normal Press-Ups 2 Crunchies 3 Squat Thrusts 4 Bench Dips 5 Normal Sit-Ups 6 Jump Squats 7 Decline Press-Ups 8 Half Sit-Ups 9 BurpeesRoisinPas encore d'évaluation
- Campusmap PDFDocument2 pagesCampusmap PDFDenis DalliPas encore d'évaluation
- ANBC Conditions of AssistanceDocument2 pagesANBC Conditions of AssistanceRoisinPas encore d'évaluation
- Trust SoundtrackDocument2 pagesTrust SoundtrackRoisinPas encore d'évaluation
- PregnancyDocument2 pagesPregnancyRoisinPas encore d'évaluation
- FitnessAssessment 2015 16 PDFDocument16 pagesFitnessAssessment 2015 16 PDFlaxave8817Pas encore d'évaluation
- n55 Australian Dietary Guidelines 130530 PDFDocument226 pagesn55 Australian Dietary Guidelines 130530 PDFtech1322Pas encore d'évaluation
- Leaflet Physical Activity Recommendations PDFDocument2 pagesLeaflet Physical Activity Recommendations PDFRoisinPas encore d'évaluation
- Folic AcidDocument2 pagesFolic AcidRoisinPas encore d'évaluation
- Delayed Onset Muscle Soreness (Doms)Document2 pagesDelayed Onset Muscle Soreness (Doms)steffiecruz06Pas encore d'évaluation
- Vegetarian Food FactsDocument2 pagesVegetarian Food FactsRoisinPas encore d'évaluation
- Starting An Exercise Program: Health and Medical Questionnaire Fitness Assessment Informed ConsentDocument2 pagesStarting An Exercise Program: Health and Medical Questionnaire Fitness Assessment Informed ConsentRoisinPas encore d'évaluation
- Trans FatsDocument2 pagesTrans FatsRoisinPas encore d'évaluation
- A Guide For Exercising During and After Treatment For Cancer PDFDocument20 pagesA Guide For Exercising During and After Treatment For Cancer PDFRoisinPas encore d'évaluation
- Files 10624pfibrosarcomaDocument4 pagesFiles 10624pfibrosarcomaLily NGPas encore d'évaluation
- Health & Fitness Journal: of CanadaDocument13 pagesHealth & Fitness Journal: of CanadaRoisinPas encore d'évaluation
- How To Work With Health Care Providers: A Systematic ApproachDocument8 pagesHow To Work With Health Care Providers: A Systematic ApproachRoisinPas encore d'évaluation
- 4 QuestionnaireDocument4 pages4 QuestionnaireRoisinPas encore d'évaluation
- Written Report - PhilHealthDocument5 pagesWritten Report - PhilHealthSophia VeralloPas encore d'évaluation
- Alternative Certificate - Foundation Competences ProtectedDocument12 pagesAlternative Certificate - Foundation Competences ProtectedFlavian Costin NacladPas encore d'évaluation
- Evaluation of Dysuria in AdultsDocument8 pagesEvaluation of Dysuria in AdultspapermintPas encore d'évaluation
- Disinfection & Sterilization 2Document49 pagesDisinfection & Sterilization 2YasminPas encore d'évaluation
- Personal Data:: Curiculum VitaeDocument7 pagesPersonal Data:: Curiculum Vitaebudi darmantaPas encore d'évaluation
- Gallbladder DiseasesDocument6 pagesGallbladder DiseasesJoharaPas encore d'évaluation
- DownloadDocument1 pageDownloadsathish KumarPas encore d'évaluation
- Manajemen Nyeri Dengan DexketoprofenDocument27 pagesManajemen Nyeri Dengan Dexketoprofenmaya santiPas encore d'évaluation
- CRE Fixed Wire Balloon Dilatation CatheterDocument2 pagesCRE Fixed Wire Balloon Dilatation CathetermaassingerPas encore d'évaluation
- Total Abdominal Hysterectomy With Bilateral SalpingoDocument3 pagesTotal Abdominal Hysterectomy With Bilateral SalpingoReyniel Pablo ElumbaPas encore d'évaluation
- Patient Admission Hospital Admission ChecklistDocument6 pagesPatient Admission Hospital Admission ChecklistSweetly MamukoPas encore d'évaluation
- Introduction To The Three-Dimensional Scoliosis Treatment According To SchrothDocument6 pagesIntroduction To The Three-Dimensional Scoliosis Treatment According To SchrothIvens NakagawaPas encore d'évaluation
- Reference Books For CSIR-NET - BioTecNikaDocument11 pagesReference Books For CSIR-NET - BioTecNikaDr-Katari VenkateshPas encore d'évaluation
- Euroline Ana Profile 23 (Igg) Test Instruction: Modifications To The Former Version Are Marked in GreyDocument16 pagesEuroline Ana Profile 23 (Igg) Test Instruction: Modifications To The Former Version Are Marked in GreyRiskullah MakmurPas encore d'évaluation
- ActinobacillosisDocument17 pagesActinobacillosisKhalid Gul100% (1)
- A Study of Cisplatin Chemoteraphy and Hearing LossDocument4 pagesA Study of Cisplatin Chemoteraphy and Hearing LossPriska AmeliaPas encore d'évaluation
- Universiti Teknologi Mara Cawangan Pahang Faculty of Sports Science & RecreationDocument26 pagesUniversiti Teknologi Mara Cawangan Pahang Faculty of Sports Science & RecreationJalal NasirPas encore d'évaluation
- Jl. Pulo Mas Timur K No.2 RT4/RW.14, Kayu Pu H, Kec. Pulo Gadung, Kota Jakarta Timur, Daerah Khusus Ibukota Jakarta 13210Document1 pageJl. Pulo Mas Timur K No.2 RT4/RW.14, Kayu Pu H, Kec. Pulo Gadung, Kota Jakarta Timur, Daerah Khusus Ibukota Jakarta 13210suherman palelePas encore d'évaluation
- ACE Inhibitors: Medications To Control Blood PressureDocument3 pagesACE Inhibitors: Medications To Control Blood PressurekPas encore d'évaluation
- Puberty (OBGYN Presentation #1)Document15 pagesPuberty (OBGYN Presentation #1)Alex KadirPas encore d'évaluation
- Isotonic, Hypotonic, and Hypertonic IV Fluid Solution: Isotonic Solutions: Contains Approximately The SameDocument1 pageIsotonic, Hypotonic, and Hypertonic IV Fluid Solution: Isotonic Solutions: Contains Approximately The SamemimPas encore d'évaluation
- Blood TransfusionDocument2 pagesBlood TransfusionKomal TomarPas encore d'évaluation
- Cefizox® FDADocument15 pagesCefizox® FDAMutiaraPas encore d'évaluation
- Uterine Septum A Case Report and A Recommendation.2Document3 pagesUterine Septum A Case Report and A Recommendation.2Sevastian GalburPas encore d'évaluation
- UAS Kritis 1 (T4) - Monitoring Fungsi Pernapasan - Bu HY (A11)Document108 pagesUAS Kritis 1 (T4) - Monitoring Fungsi Pernapasan - Bu HY (A11)rifqifuadiPas encore d'évaluation
- CHOLECYSTECTOMYDocument3 pagesCHOLECYSTECTOMYlovelysummerPas encore d'évaluation