Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Asme B16.34Document15 pagesAsme B16.34Achraf Ismail100% (1)
- UNICEF Conceptual Framework of MalnutritionDocument4 pagesUNICEF Conceptual Framework of MalnutritionAyu Putri Noviyanti100% (2)
- Basics of Cycling TrainingDocument19 pagesBasics of Cycling Trainingmodulofriki100% (4)
- LESSON 1 Grade 11 August 18,2021Document17 pagesLESSON 1 Grade 11 August 18,2021Jasmine Erika L. Do-omaPas encore d'évaluation
- Iassacon 2018 SP 23022018 Finalwithouthall 2 Ic 6Document4 pagesIassacon 2018 SP 23022018 Finalwithouthall 2 Ic 6ishu sPas encore d'évaluation
- BADOLEDocument46 pagesBADOLESadiya MohammedPas encore d'évaluation
- 30 Minute FitnessDocument7 pages30 Minute FitnessMuthu NagarajanPas encore d'évaluation
- Seal of Healthy Barangay IndicatorDocument2 pagesSeal of Healthy Barangay IndicatorBarangay PitaPas encore d'évaluation
- Fitness Component Study GuideDocument3 pagesFitness Component Study Guideapi-359231347Pas encore d'évaluation
- Metabolic Training The Ultimate Guide To The Ultimate Workout (John Graham, Michael Barnes) (Z-Library)Document297 pagesMetabolic Training The Ultimate Guide To The Ultimate Workout (John Graham, Michael Barnes) (Z-Library)Andreea Slavoaca100% (1)
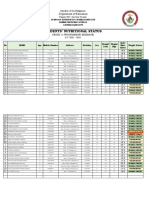
- Students Nutritional Status Template 1Document4 pagesStudents Nutritional Status Template 1Jeffreynald Arante FranciscoPas encore d'évaluation
- Monografi Asam AskorbatDocument5 pagesMonografi Asam AskorbatHeriyantiPas encore d'évaluation
- DB Only PlaybookDocument24 pagesDB Only Playbookareo.barPas encore d'évaluation
- Health Awareness ProgrammeDocument39 pagesHealth Awareness ProgrammeB. Anil KumarPas encore d'évaluation
- Case Study On Gas Station Enviromental Qualitative Risk AssessmentDocument13 pagesCase Study On Gas Station Enviromental Qualitative Risk AssessmentAlex BmxPas encore d'évaluation
- Ns Baseline Pulong Duhat Ps Sy 2023 2024Document2 pagesNs Baseline Pulong Duhat Ps Sy 2023 2024CATHERINE RAYOPas encore d'évaluation
- Eap 5 Assignment Cover Sheet: ClassDocument8 pagesEap 5 Assignment Cover Sheet: ClassThu MinhPas encore d'évaluation
- 2022-03-12 New Scientist - Battle of The Mid-Life Bulge PDFDocument4 pages2022-03-12 New Scientist - Battle of The Mid-Life Bulge PDFRyan HoangPas encore d'évaluation
- MalnutritionDocument29 pagesMalnutritionMohd Sameer KhanPas encore d'évaluation
- Classification of VitaminsDocument3 pagesClassification of VitaminsHabiba's WorldPas encore d'évaluation
- Malnutrition 1Document30 pagesMalnutrition 1Kazama08Pas encore d'évaluation
- Essay Hook ExampleDocument5 pagesEssay Hook Exampled3gpmvqwPas encore d'évaluation
- Jurnal Sampah Unri PDFDocument11 pagesJurnal Sampah Unri PDFarisPas encore d'évaluation
- Running NutritionDocument42 pagesRunning NutritionAlejandro JustoPas encore d'évaluation
- Sleep Rest PatternDocument4 pagesSleep Rest PatternCindy DelfinPas encore d'évaluation
- Cnursing Care Plan MonteronDocument6 pagesCnursing Care Plan MonteronCharlene Grace ReginoPas encore d'évaluation
- A New Discovery Revealed : The 24-Hour Diet Is HERE!Document3 pagesA New Discovery Revealed : The 24-Hour Diet Is HERE!fumiPas encore d'évaluation
- Peaking For PowerliftingDocument20 pagesPeaking For PowerliftingOssaBluPas encore d'évaluation
- Workplace Safety & Health Guidelines: Fatigue ManagementDocument21 pagesWorkplace Safety & Health Guidelines: Fatigue ManagementShajita DPas encore d'évaluation
- Octagonal Warning Labels Perform Best in Helping Consumers Choose Healthier Food, Major Study in Jamaica ShowsDocument3 pagesOctagonal Warning Labels Perform Best in Helping Consumers Choose Healthier Food, Major Study in Jamaica ShowsGail HoadPas encore d'évaluation