Vous aimerez peut-être aussi
- RPD M C Q With AnswersDocument23 pagesRPD M C Q With Answersيارا حسين81% (16)
- TechTalk HemolysisDocument2 pagesTechTalk HemolysisARIF AHAMMED P0% (1)
- Lesson-09 MODUL PDFDocument9 pagesLesson-09 MODUL PDFanggaririn100% (1)
- CSF Analysis AFP 2021Document9 pagesCSF Analysis AFP 2021henry leonardo gaona pinedaPas encore d'évaluation
- Data Interpretation For Medical StudentDocument18 pagesData Interpretation For Medical StudentWee K WeiPas encore d'évaluation
- Blood Firm CommentDocument14 pagesBlood Firm Commentmaxwell amponsahPas encore d'évaluation
- Manejo de Muestras HemolizadasDocument22 pagesManejo de Muestras Hemolizadaspintopablo108bPas encore d'évaluation
- Fluid CytologyDocument132 pagesFluid CytologySeby SebastianPas encore d'évaluation
- Fluid Cytology BookDocument129 pagesFluid Cytology Bookpooo80100% (1)
- Lippi 2018Document6 pagesLippi 2018Harika PutraPas encore d'évaluation
- Inferior Vena Cava Ultrasonography For Volume Status EvaluationDocument13 pagesInferior Vena Cava Ultrasonography For Volume Status Evaluationtavo570Pas encore d'évaluation
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDocument9 pagesThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnPas encore d'évaluation
- Avian Blood Collection and Hematology - WSAVA 2015 Congress - VINDocument4 pagesAvian Blood Collection and Hematology - WSAVA 2015 Congress - VINMustafa AL-AsadsyPas encore d'évaluation
- 2018 FluidcytoDocument143 pages2018 FluidcytoAdriana GîrboanPas encore d'évaluation
- Haematologist-Reviewed Peripheral Blood Smear in PDocument6 pagesHaematologist-Reviewed Peripheral Blood Smear in PElba AlvarezPas encore d'évaluation
- A Manual of Laboratory Techniques in Clinical Hematology 1Document15 pagesA Manual of Laboratory Techniques in Clinical Hematology 1Jaycel Mae Ba-ay (Gaikokujinn)Pas encore d'évaluation
- 3minute Blood Film EvaluationsDocument16 pages3minute Blood Film EvaluationsSanthi Swetha100% (1)
- Full Blood Count Apr04, DR Eva RaikDocument7 pagesFull Blood Count Apr04, DR Eva RaikDanielcc LeePas encore d'évaluation
- Preface CLLDocument3 pagesPreface CLLhajar.wishPas encore d'évaluation
- Cost Analysis of A Neonatal Point-of-Care MonitorDocument10 pagesCost Analysis of A Neonatal Point-of-Care MonitorMARIO LOPEZ VILLAMILPas encore d'évaluation
- Review On Blood Culture: Anup R Warrier, Mathew ThomasDocument3 pagesReview On Blood Culture: Anup R Warrier, Mathew Thomaspurnima4uonlyPas encore d'évaluation
- Pancytopenia A Clinico Hematological StudyDocument6 pagesPancytopenia A Clinico Hematological StudyUci Rahmadhani MPas encore d'évaluation
- HTTPS://WWW Scribd com/document/374501075/MAKALAH-IMUNOSEROLOGIDocument4 pagesHTTPS://WWW Scribd com/document/374501075/MAKALAH-IMUNOSEROLOGIRifky WahyullahPas encore d'évaluation
- An Etiological Reappraisal of Pancytopenia - LargestDocument9 pagesAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaPas encore d'évaluation
- Peripheral Blood Smear Pathologist ToolDocument3 pagesPeripheral Blood Smear Pathologist ToolSimon HafeniPas encore d'évaluation
- Clinico - Hematological Analysis of Pancytopenia: A Bone Marrow StudyDocument6 pagesClinico - Hematological Analysis of Pancytopenia: A Bone Marrow StudySrinath M VPas encore d'évaluation
- ICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersDocument22 pagesICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersSofia BujosaPas encore d'évaluation
- ICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersDocument22 pagesICSH Guidelines For The Laboratory Diagnosis of Nonimmune Hereditary Red Cell Membrane DisordersSofia BujosaPas encore d'évaluation
- DX de Las Enfermedades No Inmunologicas de La Membrana Del EritorcitoDocument22 pagesDX de Las Enfermedades No Inmunologicas de La Membrana Del EritorcitoMiguel Angel Hernandez SerratoPas encore d'évaluation
- Performance of CellaVision DM96 in Leukocyte ClassificationDocument5 pagesPerformance of CellaVision DM96 in Leukocyte ClassificationarielPas encore d'évaluation
- Matson 1961Document4 pagesMatson 1961NyimasPas encore d'évaluation
- Hematology 1 Lab - The Reticulocyte CountDocument17 pagesHematology 1 Lab - The Reticulocyte CountCIRILO MABBORANGPas encore d'évaluation
- Efficacy of Ascitic Acid Dipstick Leukocyte Esterase Activity in Early Diagnosis of Spontaneous Bacterial PeritonitisDocument6 pagesEfficacy of Ascitic Acid Dipstick Leukocyte Esterase Activity in Early Diagnosis of Spontaneous Bacterial PeritonitisIJAR JOURNALPas encore d'évaluation
- Int J Lab Hematology - 2021 - Kitchen - International Council For Standardization in Haematology ICSH Recommendations ForDocument12 pagesInt J Lab Hematology - 2021 - Kitchen - International Council For Standardization in Haematology ICSH Recommendations ForLaboratorium RS BELLAPas encore d'évaluation
- 8584-Article Text-31293-1-10-20110913Document5 pages8584-Article Text-31293-1-10-20110913Maksudur Rahman ShawonPas encore d'évaluation
- Pjms 29 1153Document5 pagesPjms 29 1153Hanshel SatriyaPas encore d'évaluation
- Efusi Pleura MaskellDocument10 pagesEfusi Pleura MaskellYessica Chrystie Dian SinurayaPas encore d'évaluation
- 2016-Yahav Et Al-Cytometry Part ADocument10 pages2016-Yahav Et Al-Cytometry Part AgiladPas encore d'évaluation
- Biochem 24 1 57 9Document12 pagesBiochem 24 1 57 9Yaser MPas encore d'évaluation
- Cerebrospinal Fluid (CSF) AnalysisDocument8 pagesCerebrospinal Fluid (CSF) AnalysisVidhya.MPas encore d'évaluation
- "Normal" Mean Corpuscular Volume Does Not Exclude The Diagnosis of ThalassaemiaDocument3 pages"Normal" Mean Corpuscular Volume Does Not Exclude The Diagnosis of ThalassaemiaTanveerPas encore d'évaluation
- Derrame Pleural 3Document46 pagesDerrame Pleural 3Héctor David GalánPas encore d'évaluation
- Recommendations For Processing of Blood Samples For Coagulation TestingDocument12 pagesRecommendations For Processing of Blood Samples For Coagulation TestingRandy HuyhuaPas encore d'évaluation
- Lmy 030Document7 pagesLmy 030Tuan NguyenPas encore d'évaluation
- 68-Year-Old Man With Fatigue, Fever, and Weight Loss PDFDocument4 pages68-Year-Old Man With Fatigue, Fever, and Weight Loss PDFRaghad Al-AnsariPas encore d'évaluation
- Bone Marrow Aplasia: A Rare Complication of Disseminated TuberculosisDocument3 pagesBone Marrow Aplasia: A Rare Complication of Disseminated TuberculosisayuPas encore d'évaluation
- 24 - Liquor AnaliseDocument6 pages24 - Liquor AnaliseomboPas encore d'évaluation
- 22 Anaesthesia HandbookDocument7 pages22 Anaesthesia HandbookHany ElbarougyPas encore d'évaluation
- Howto Companion August2009Document4 pagesHowto Companion August2009lybrakissPas encore d'évaluation
- Adult Blood Culture Guideline Updated Sept2016Document3 pagesAdult Blood Culture Guideline Updated Sept2016Dima GheorghePas encore d'évaluation
- Diagnostics 10 01046 v2Document20 pagesDiagnostics 10 01046 v2M Halis HermawanPas encore d'évaluation
- CaravagioDocument9 pagesCaravagiomohamed baba ahmedPas encore d'évaluation
- Digital Microscopy As A Screening Tool For The Diagnosis of Hereditary Hemolytic AnemiaDocument10 pagesDigital Microscopy As A Screening Tool For The Diagnosis of Hereditary Hemolytic AnemiaRanhie Pen'ned CendhirhiePas encore d'évaluation
- The Divergent Morphological Classification of VariDocument3 pagesThe Divergent Morphological Classification of VariKai HavertzPas encore d'évaluation
- Chapter 5 Hemolysis Lipemia and High Bilirubin Effect On Laboratory Tests 2013 Accurate Results in The Clinical LaboratoryDocument10 pagesChapter 5 Hemolysis Lipemia and High Bilirubin Effect On Laboratory Tests 2013 Accurate Results in The Clinical LaboratoryCristina Gaidargi100% (1)
- Feline Blood Film 230902 043358Document13 pagesFeline Blood Film 230902 04335897namithaPas encore d'évaluation
- 4 Pleural, Pericardial, and Peritoneal FluidDocument25 pages4 Pleural, Pericardial, and Peritoneal FluidnanxtoyahPas encore d'évaluation
- Pleuralfluidbiomarkers: Beyond The Light CriteriaDocument11 pagesPleuralfluidbiomarkers: Beyond The Light CriteriaVijay KumarPas encore d'évaluation
- Fast Facts: Myelofibrosis: Reviewed by Professor Ruben A. MesaD'EverandFast Facts: Myelofibrosis: Reviewed by Professor Ruben A. MesaPas encore d'évaluation
- Diagnosis of Blood and Bone Marrow DisordersD'EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangPas encore d'évaluation
- Best Practices of Apheresis in Hematopoietic Cell TransplantationD'EverandBest Practices of Apheresis in Hematopoietic Cell TransplantationSyed A. AbutalibPas encore d'évaluation
- Goldberg 1970Document8 pagesGoldberg 1970Ria Rizki JayantiPas encore d'évaluation
- Gambaran Angka Kejadian, Karakteristik Dan Ekspertise Radiologi USG Pasien Asites Di RS Al-Ihsan Periode 2013-2015Document6 pagesGambaran Angka Kejadian, Karakteristik Dan Ekspertise Radiologi USG Pasien Asites Di RS Al-Ihsan Periode 2013-2015Ria Rizki JayantiPas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar PustakaRia Rizki JayantiPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptRia Rizki JayantiPas encore d'évaluation
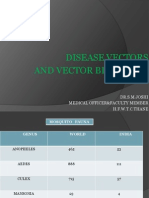
- Disease Vectors and Vector BionomicsDocument16 pagesDisease Vectors and Vector BionomicsSuhas JoshiPas encore d'évaluation
- Sufixe Si PrefixeDocument14 pagesSufixe Si Prefixeseaofdreams6Pas encore d'évaluation
- English Sistem EndocrineDocument9 pagesEnglish Sistem EndocrineNurlaili YaniPas encore d'évaluation
- Dengue Fever and PregnancyDocument6 pagesDengue Fever and PregnancyImanuel Far-FarPas encore d'évaluation
- Fluoride Toxicity and DefluoridationDocument91 pagesFluoride Toxicity and DefluoridationAbhijeet Kadu50% (2)
- RNTCP India - Training Module (Dec - 2010) For Medical OfficersDocument128 pagesRNTCP India - Training Module (Dec - 2010) For Medical OfficersDr.Sagindar100% (1)
- Sci Quiz MusculoskeletalDocument16 pagesSci Quiz MusculoskeletalJERVES FALCOTELOPas encore d'évaluation
- DR Deagle's H1N1 ReportDocument61 pagesDR Deagle's H1N1 Reportkingofswords100% (1)
- 5090 s16 Ms 22 PDFDocument10 pages5090 s16 Ms 22 PDFclydePas encore d'évaluation
- Housing Systems of PoultryDocument7 pagesHousing Systems of PoultryferdinandPas encore d'évaluation
- Professional Anesthesia HandbookDocument114 pagesProfessional Anesthesia HandbookSooryajith DineshPas encore d'évaluation
- Kingdom AnimaliaDocument3 pagesKingdom AnimaliaLloydDagsil100% (1)
- Anatomy From The DoctorDocument208 pagesAnatomy From The DoctorSweet manPas encore d'évaluation
- HistologyDocument18 pagesHistologyGlavinorPas encore d'évaluation
- Jump To Navigation Jump To Search: For Other Uses, SeeDocument19 pagesJump To Navigation Jump To Search: For Other Uses, SeeDanny FentomPas encore d'évaluation
- Types of FeverDocument16 pagesTypes of Fevercute_ildz0% (1)
- ECG Interpretation BookDocument57 pagesECG Interpretation BookLouis Plan100% (2)
- Correlative AnatomyDocument19 pagesCorrelative AnatomyLicensed to HealPas encore d'évaluation
- Practice English ConconantsDocument17 pagesPractice English ConconantsStella Trendafilova0% (1)
- ACT H Cracked Nipples FactSheet 2018-V1Document2 pagesACT H Cracked Nipples FactSheet 2018-V1dhea handyaraPas encore d'évaluation
- PHD Research ProposalDocument8 pagesPHD Research ProposalMalik Ijaz Khan100% (1)
- A Myth About Anastomotic LeakDocument3 pagesA Myth About Anastomotic LeakAvinash RoyPas encore d'évaluation
- 0610 m16 Ms 42Document10 pages0610 m16 Ms 42Keshav JindalPas encore d'évaluation
- Food Borne Diseases and Its PreventionDocument181 pagesFood Borne Diseases and Its Preventionapi-19916399Pas encore d'évaluation
- Presentation About CellsDocument39 pagesPresentation About Cellsharfiyanto100% (2)
- n6 Andrzej Sapkowski Season - of - StormsDocument9 pagesn6 Andrzej Sapkowski Season - of - StormsRazvan Visoiu0% (2)
- MER 2.0.0 Indicator Reference GuideDocument174 pagesMER 2.0.0 Indicator Reference GuideMigori Art DataPas encore d'évaluation
- NEET UG Biology Reproductive HealthDocument13 pagesNEET UG Biology Reproductive Healthritik SharmaPas encore d'évaluation
- Presentation On Agriculture & Animal HusbandryDocument12 pagesPresentation On Agriculture & Animal HusbandryVijay Narayan Yadav0% (1)