Vous aimerez peut-être aussi
- Longwall Mining at Shallow Depth of Cover in IndiaD'EverandLongwall Mining at Shallow Depth of Cover in IndiaPas encore d'évaluation
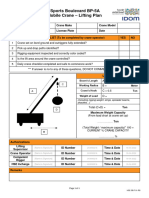
- Crane Lift Plan: 1. Project Data Page 1 of 2Document2 pagesCrane Lift Plan: 1. Project Data Page 1 of 2Ένκινουαν Κόγκ ΑδάμουPas encore d'évaluation
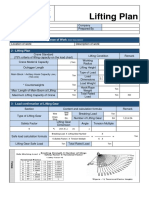
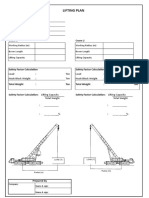
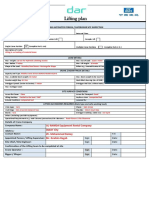
- Lifting PlanDocument2 pagesLifting PlanMidhunRameshThuvasseryPas encore d'évaluation
- Critical Lift Worksheet: Crane Information Lift InformationDocument2 pagesCritical Lift Worksheet: Crane Information Lift InformationCarlos Chacin APas encore d'évaluation
- Critical Lift Plan FormDocument1 pageCritical Lift Plan FormMuhammad Afif MansorPas encore d'évaluation
- Critical Lifting Plan 10T, 80% Capacity, One Side 10m: Al-Dur Ii Iwpp ProjectDocument1 pageCritical Lifting Plan 10T, 80% Capacity, One Side 10m: Al-Dur Ii Iwpp ProjectJianping KePas encore d'évaluation
- EDCINTL - hse.FM.080.R4-Critical Lift Permit Crane ADocument2 pagesEDCINTL - hse.FM.080.R4-Critical Lift Permit Crane ABogdan-Gabriel SchiopuPas encore d'évaluation
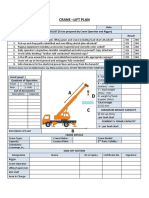
- Crane Lift PlanDocument4 pagesCrane Lift Planabdalla el-saadaneyPas encore d'évaluation
- Critical Lift WorksheetDocument2 pagesCritical Lift WorksheetPatrick ChambersPas encore d'évaluation
- Form 5068A Crane Use Planning Process REV 2015Document4 pagesForm 5068A Crane Use Planning Process REV 2015Samuel LumbanrajaPas encore d'évaluation
- Critical Lift PermitDocument1 pageCritical Lift PermitEduardo SanchezPas encore d'évaluation
- Lifting PlanDocument9 pagesLifting Plansatyabrath dhalPas encore d'évaluation
- Lift Plan - Routine - Updated-October. 2017 - Rev 01Document1 pageLift Plan - Routine - Updated-October. 2017 - Rev 01sudeesh kumarPas encore d'évaluation
- Critical Lift Plan Form: Do Not Leave Any Blank Spaces On This Form!Document9 pagesCritical Lift Plan Form: Do Not Leave Any Blank Spaces On This Form!ARULSELVAN MURUGESANPas encore d'évaluation
- Lifting PlanDocument1 pageLifting PlanZubair KhawarPas encore d'évaluation
- Referensi Rigging PlanDocument4 pagesReferensi Rigging PlanLaurentius CalvinPas encore d'évaluation
- Project Lifting Plan (Rev 00)Document10 pagesProject Lifting Plan (Rev 00)M AzharPas encore d'évaluation
- 37 Lifting PlanDocument1 page37 Lifting PlanP.M.K anthPas encore d'évaluation
- Level 3 Critical Lifting PlanDocument6 pagesLevel 3 Critical Lifting PlanMARDOULI YOUSSEFPas encore d'évaluation
- LSH Best Builder SDN BHD: Project: LSH Taman Segar Crane: (T) ModelDocument3 pagesLSH Best Builder SDN BHD: Project: LSH Taman Segar Crane: (T) ModelimranPas encore d'évaluation
- Crane Lift PlanDocument3 pagesCrane Lift PlandammyPas encore d'évaluation
- Mobile Crane Lifting PlanDocument1 pageMobile Crane Lifting PlanazozinlcPas encore d'évaluation
- Lifting PlanDocument2 pagesLifting PlanDoo PLTGU86% (37)
- Lift Worksheet PDFDocument1 pageLift Worksheet PDFChristian BulaongPas encore d'évaluation
- 3-Pre-Lift Checklist Rev A 06302015Document2 pages3-Pre-Lift Checklist Rev A 06302015Zubair Ahmed Khaskheli100% (1)
- Appendix G Crane Safety Attachment A Pre Lift PlanDocument2 pagesAppendix G Crane Safety Attachment A Pre Lift PlanSyed Waqhas0% (1)
- Petroleum Development Oman: Lift Plan For Lifting OperationDocument7 pagesPetroleum Development Oman: Lift Plan For Lifting OperationVuthpalachaitanya KrishnaPas encore d'évaluation
- MJ Bro CriticalDocument1 pageMJ Bro CriticalRajanna NallaPas encore d'évaluation
- Crane Lift PlanDocument1 pageCrane Lift PlanHamid Ali100% (5)
- Lifting Plan FormDocument3 pagesLifting Plan FormFahrul Andi100% (4)
- HSE-TP-102-C Lifting Plan Using Mobile CraneDocument13 pagesHSE-TP-102-C Lifting Plan Using Mobile CraneSyed Fawad ShahPas encore d'évaluation
- 3-Pre-Lift Checklist Rev A 06302015Document4 pages3-Pre-Lift Checklist Rev A 06302015Bruce FerreiraPas encore d'évaluation
- Mobile Crane PermitDocument2 pagesMobile Crane PermitSaumya Siddhantha ChoudhuryPas encore d'évaluation
- Lifting PlanDocument2 pagesLifting Plansujith s p100% (2)
- Lifting Plan For UnloadingDocument5 pagesLifting Plan For Unloadingkhaled redaPas encore d'évaluation
- Appendix - Nlng-lp-017 - Lift Plan For Lifting and Installation of Roof Trusses of Amenities Building (19418) - Comments From MosesDocument32 pagesAppendix - Nlng-lp-017 - Lift Plan For Lifting and Installation of Roof Trusses of Amenities Building (19418) - Comments From MosesAdebayo M JayeolaPas encore d'évaluation
- SSA FormDocument1 pageSSA FormFarid AlilouchePas encore d'évaluation
- Lifting Plan TemplateDocument16 pagesLifting Plan TemplatezwvvsoPas encore d'évaluation
- Serious Lift Calculation and Authorization FormDocument2 pagesSerious Lift Calculation and Authorization FormAbdulKather100% (1)
- Mobile Crane Lifting PermitDocument1 pageMobile Crane Lifting PermitWaqas IslamPas encore d'évaluation
- FM-OHS-1300-02 Lift Plan - Mobile Crane R01Document4 pagesFM-OHS-1300-02 Lift Plan - Mobile Crane R01CosminZbirnaPas encore d'évaluation
- BP TGH PF TR B 0020a - 022 e 1002b - by Crane 200te (BPP Puller)Document36 pagesBP TGH PF TR B 0020a - 022 e 1002b - by Crane 200te (BPP Puller)Abdul Majid ZPas encore d'évaluation
- Mobile Crane Lifting Plan - Routine Operation1Document2 pagesMobile Crane Lifting Plan - Routine Operation1Becha MouradPas encore d'évaluation
- LP 1T Pipes Critical Crane Lift Plan 25T Crane CPFDocument1 pageLP 1T Pipes Critical Crane Lift Plan 25T Crane CPFMPS PSKPas encore d'évaluation
- Lifting Operation Permit - NCC-Project Seabird Phase IIA, DB-03Document1 pageLifting Operation Permit - NCC-Project Seabird Phase IIA, DB-03Farman ShaikhPas encore d'évaluation
- Lifting PlanDocument3 pagesLifting PlanabdulrahimabrahmanPas encore d'évaluation
- CLP 1 & CLP2 Critical Lift Plan (350T & 100T)Document2 pagesCLP 1 & CLP2 Critical Lift Plan (350T & 100T)babjihanumanthu100% (2)
- Lifting Plan Registration PDFDocument1 pageLifting Plan Registration PDFScribdTranslationsPas encore d'évaluation
- Lifting Operation PlanDocument1 pageLifting Operation PlanMelchor MolinoPas encore d'évaluation
- Lifting Permit ImexDocument2 pagesLifting Permit Imexsophia sambaPas encore d'évaluation
- Lifting Plan For 62.07 RepairDocument6 pagesLifting Plan For 62.07 RepairLaith Salman100% (1)
- Ground Bearing PressureDocument5 pagesGround Bearing PressureMartin Haposan SiahaanPas encore d'évaluation
- NRCLP 223Document5 pagesNRCLP 223Ali AlahmaPas encore d'évaluation
- Heavy Lift PresentationDocument94 pagesHeavy Lift Presentationkarthika18maniPas encore d'évaluation
- Lifting Plan: Lifting Appointed Person / Supervisor Site InspectionDocument4 pagesLifting Plan: Lifting Appointed Person / Supervisor Site Inspectionkhaled redaPas encore d'évaluation
- 015-Lifting Plan Method & Risk AssessmentDocument3 pages015-Lifting Plan Method & Risk AssessmentSarabjit Singh SanghaPas encore d'évaluation
- Lifting PermitDocument1 pageLifting PermitManesh MPas encore d'évaluation
- Pre-Lift Check List: A Toshiba America Energy Systems CompanyDocument2 pagesPre-Lift Check List: A Toshiba America Energy Systems Companyr afriantoPas encore d'évaluation
- Crane Lift Plan: Company Name Project: ClientDocument5 pagesCrane Lift Plan: Company Name Project: Clientscottie Mailau100% (1)
- Baby DragonDocument8 pagesBaby DragonAnaJúlia100% (2)
- Haaaaaaaaaaaaaaaaaaaaaaaaaaaaaa AaaaaaaaaaaaaaaDocument10 pagesHaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa AaaaaaaaaaaaaaaJuliastikaPuspaningtyasPas encore d'évaluation
- SB-104 SSB Transceiver - Operation Manual - Heathkit.1974.166sDocument166 pagesSB-104 SSB Transceiver - Operation Manual - Heathkit.1974.166sJose Luis Sesma100% (2)
- Swiggy Business Model CanvasDocument2 pagesSwiggy Business Model CanvasBharatGambhir100% (1)
- Scene 0312Document124 pagesScene 0312Sydney F. Sarachan100% (1)
- ClothesDocument2 pagesClothesminka_82Pas encore d'évaluation
- DB CalculationsDocument6 pagesDB CalculationsJenny ArutaPas encore d'évaluation
- Pass Res B1plus UT 1ADocument2 pagesPass Res B1plus UT 1AKarolina PelcPas encore d'évaluation
- Bridge and Tower Quiz PDFDocument4 pagesBridge and Tower Quiz PDFapi-234877943Pas encore d'évaluation
- The Lord of The Rings - IntroductionDocument1 pageThe Lord of The Rings - IntroductionblackpichaPas encore d'évaluation
- Dsdhi LM55 F400 C4Document2 pagesDsdhi LM55 F400 C4Manuel CastilloPas encore d'évaluation
- Service ManualDocument9 pagesService ManualgibonulPas encore d'évaluation
- How To Draw Noir Comics The Art and Technique of Visual Storytelling PDFDocument5 pagesHow To Draw Noir Comics The Art and Technique of Visual Storytelling PDFgordon0% (5)
- Els MatrixDocument6 pagesEls MatrixJade BaliolaPas encore d'évaluation
- Select Hollow Blade TurbineDocument10 pagesSelect Hollow Blade TurbinescranderiPas encore d'évaluation
- Halloween HistoryDocument2 pagesHalloween Historyapi-169100738Pas encore d'évaluation
- HOPE 3 Lesson 1 Elements of DanceDocument29 pagesHOPE 3 Lesson 1 Elements of DanceJay El Taypin OrdanezaPas encore d'évaluation
- In Touch - August 1, 2016 USA PDFDocument76 pagesIn Touch - August 1, 2016 USA PDFSabina FloreaPas encore d'évaluation
- Cornell Note Questions For Great Gatsby Chapters 1-3Document2 pagesCornell Note Questions For Great Gatsby Chapters 1-3Julia Abreu100% (1)
- Cleaning Equipments: Types of BroomsDocument8 pagesCleaning Equipments: Types of BroomsSushma MurthyPas encore d'évaluation
- HP ZD7000 PDFDocument192 pagesHP ZD7000 PDFbarqzr daviPas encore d'évaluation
- Subwoofer Box 6.5 Inch Subwoofer Ported Box Pipe9Document2 pagesSubwoofer Box 6.5 Inch Subwoofer Ported Box Pipe9Arif Kurniawan HidayatPas encore d'évaluation
- Work 1 Free BTCDocument22 pagesWork 1 Free BTCYan MikhlinPas encore d'évaluation
- GDDocument1 pageGDMichelle NuarinPas encore d'évaluation
- Revised ResumeDocument2 pagesRevised Resumeapi-312360514Pas encore d'évaluation
- Processor Operating System Memory GPUDocument4 pagesProcessor Operating System Memory GPUEDWARD JOSEPH D. MACOSEPas encore d'évaluation
- Duration, Location and Toss: by LawsDocument7 pagesDuration, Location and Toss: by LawsVatigersPas encore d'évaluation
- The Singing SilenceDocument5 pagesThe Singing Silencetishalikhar7Pas encore d'évaluation
- 19TH0257 - 3RD Year - 5TH Sem - CHT - Internal-01Document11 pages19TH0257 - 3RD Year - 5TH Sem - CHT - Internal-01DHANASEENUVASAN DPas encore d'évaluation
- DDI Dimensional Imaging DI3DDocument4 pagesDDI Dimensional Imaging DI3DgildsonrjPas encore d'évaluation