Vous aimerez peut-être aussi
- The Human Side of MedicineDocument300 pagesThe Human Side of Medicinetamikanji100% (1)
- ESRD Case Analysis - Group 4Document34 pagesESRD Case Analysis - Group 4Sean Jeffrey J. FentressPas encore d'évaluation
- Pephysical FitnessDocument44 pagesPephysical FitnessBasil Francis Alajid77% (13)
- Nutrition and Diet Therapy: Principles and PracticeDocument11 pagesNutrition and Diet Therapy: Principles and PracticeCharisse Arriane BelasotoPas encore d'évaluation
- Type 2 Diabetes MellitusDocument19 pagesType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Refeeding Syndrome Current Opinion 2020Document5 pagesRefeeding Syndrome Current Opinion 2020Pedro Paulo GuerraPas encore d'évaluation
- Wilson Disease - Treatment and Prognosis - UpToDateDocument13 pagesWilson Disease - Treatment and Prognosis - UpToDatericanoy191Pas encore d'évaluation
- Physiology Comprehensive Exam Pointers PDFDocument108 pagesPhysiology Comprehensive Exam Pointers PDFRaynalynGimoros100% (1)
- Anorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateDocument10 pagesAnorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDatethelesphol pascalPas encore d'évaluation
- Anorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateDocument11 pagesAnorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateAlejandra GarcíaPas encore d'évaluation
- Anorexia Nervosa - Refeeding SyndromeDocument5 pagesAnorexia Nervosa - Refeeding SyndromeDimitrios AmorgianosPas encore d'évaluation
- Refeeding SyndromeDocument10 pagesRefeeding SyndromeEstefany GonzalezPas encore d'évaluation
- Refeeding Syndrome A Literature Review KhanDocument7 pagesRefeeding Syndrome A Literature Review Khangw060qpy100% (1)
- Type 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsDocument6 pagesType 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsTrifosa Ika Septiana EryaniPas encore d'évaluation
- Hepatic Encephalopathy in Adults: Treatment (Uptodate)Document35 pagesHepatic Encephalopathy in Adults: Treatment (Uptodate)kabulkabulovich5Pas encore d'évaluation
- Medical Nutrition Therapy For Hemodialysis PatientsDocument24 pagesMedical Nutrition Therapy For Hemodialysis Patientsraquelt_65Pas encore d'évaluation
- Review Article: Refeeding Syndrome: A Literature ReviewDocument7 pagesReview Article: Refeeding Syndrome: A Literature ReviewJames Cojab SacalPas encore d'évaluation
- Acute Liver Failure in Adults - Management and Prognosis - UpToDateDocument36 pagesAcute Liver Failure in Adults - Management and Prognosis - UpToDateandus007Pas encore d'évaluation
- JCM 8071042Document17 pagesJCM 8071042Ma José EstébanezPas encore d'évaluation
- EssayDocument16 pagesEssayLorenz Sagayaga ListaPas encore d'évaluation
- Refeeding Syndrome GuidelineDocument5 pagesRefeeding Syndrome GuidelinePejman AhmadiPas encore d'évaluation
- Credo Saved Results From 2021-09-22 - From Credo ReferenceDocument4 pagesCredo Saved Results From 2021-09-22 - From Credo ReferenceAnnie JnePas encore d'évaluation
- PIIS2405457716301917Document2 pagesPIIS2405457716301917Abbas AmirPas encore d'évaluation
- Metabolic Changes Associated With Antipsychotic Use: Joseph A. Lieberman, III, M.D., M.P.HDocument6 pagesMetabolic Changes Associated With Antipsychotic Use: Joseph A. Lieberman, III, M.D., M.P.HMerlintaPas encore d'évaluation
- Hyponatremia 2015Document19 pagesHyponatremia 2015gastonsaloPas encore d'évaluation
- Journal Pre-Proof: Clinical NutritionDocument19 pagesJournal Pre-Proof: Clinical NutritionThay SousaPas encore d'évaluation
- Perioperative Management of The Diabetic PatientDocument9 pagesPerioperative Management of The Diabetic PatientFauzi Abdillah SusmanPas encore d'évaluation
- DD Metabolic SyndromeDocument5 pagesDD Metabolic SyndromeEluPas encore d'évaluation
- Reye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument7 pagesReye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreePas encore d'évaluation
- Review of The Refeeding SyndromeDocument10 pagesReview of The Refeeding SyndromelootyPas encore d'évaluation
- A Primer For The Primary Care Physician.: Drug Management in The Elderly Adult With Chronic Kidney DiseaseDocument33 pagesA Primer For The Primary Care Physician.: Drug Management in The Elderly Adult With Chronic Kidney Diseaseyuliana160793Pas encore d'évaluation
- Assessing Nutrition in Patients With Chronic Kidney Disease by Kimberly Thompson, MS, RD, LDNDocument23 pagesAssessing Nutrition in Patients With Chronic Kidney Disease by Kimberly Thompson, MS, RD, LDNCarlos RaiolPas encore d'évaluation
- Nutritional Consequences of DiseaseDocument3 pagesNutritional Consequences of DiseasesivaPas encore d'évaluation
- CHAP 2 Edit Final (1) - DevocionDocument10 pagesCHAP 2 Edit Final (1) - Devociontsam127Pas encore d'évaluation
- HypokalemiaDocument7 pagesHypokalemiaMays OthmanPas encore d'évaluation
- Jurnal Krisis AdrenalDocument4 pagesJurnal Krisis AdrenalMelda IndrawatiPas encore d'évaluation
- CaseDocument7 pagesCaseDenny EmiliusPas encore d'évaluation
- All About Anorexia in The Elderly: Czeresna H. SoejonoDocument5 pagesAll About Anorexia in The Elderly: Czeresna H. SoejonoJalu PanjongkoPas encore d'évaluation
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in AdultsDocument17 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adultsjoseaugustorojas9414Pas encore d'évaluation
- Prescribing For The ElderlyDocument8 pagesPrescribing For The ElderlykarladeyPas encore d'évaluation
- Malnutrition in Stroke PatientDocument8 pagesMalnutrition in Stroke PatientFetria MelaniPas encore d'évaluation
- HF in ElderlyDocument3 pagesHF in ElderlyHadi M.WPas encore d'évaluation
- 1179 Full PDFDocument10 pages1179 Full PDFSonia RogersPas encore d'évaluation
- Heart Failure in Patients With Metabolic Syndrome XDocument12 pagesHeart Failure in Patients With Metabolic Syndrome XErwin SiahaanPas encore d'évaluation
- 1 s2.0 S0085253815560973 MainDocument12 pages1 s2.0 S0085253815560973 MainTri Veny AfrePas encore d'évaluation
- Hypomagnesemia A Clinical Approach in Chronically Ill Patients With Multiple ComorbiditiesDocument14 pagesHypomagnesemia A Clinical Approach in Chronically Ill Patients With Multiple ComorbiditiesAthenaeum Scientific PublishersPas encore d'évaluation
- Endocrine and Metabolic EmergenciesDocument320 pagesEndocrine and Metabolic EmergenciesReem Ben Omran100% (1)
- Nutritional Status and Dietary Guidelines of Predialytic and Hemodialytic PatientsDocument138 pagesNutritional Status and Dietary Guidelines of Predialytic and Hemodialytic PatientsAndre SantePas encore d'évaluation
- Diet, Exercise, Metabolic SyndromeDocument9 pagesDiet, Exercise, Metabolic SyndromeJason WongPas encore d'évaluation
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataPas encore d'évaluation
- Nutrients: Backstage of Eating Disorder-About The Biological Mechanisms Behind The Symptoms of Anorexia NervosaDocument32 pagesNutrients: Backstage of Eating Disorder-About The Biological Mechanisms Behind The Symptoms of Anorexia NervosaMuh Rahmadan APas encore d'évaluation
- Dka Hhs RhabdoDocument5 pagesDka Hhs Rhabdohedgehog5288Pas encore d'évaluation
- Diabetesand Ramadan Update New Guidelines 2023Document4 pagesDiabetesand Ramadan Update New Guidelines 2023Taufiqurrokhman RofiiPas encore d'évaluation
- Stroke Rehabilitation. 2. Comorbidities and Complications: Elliot J. Roth, MD Stephen F. Noll, MD Abstract. RothDocument5 pagesStroke Rehabilitation. 2. Comorbidities and Complications: Elliot J. Roth, MD Stephen F. Noll, MD Abstract. RothInga HarghelPas encore d'évaluation
- MYOCARDIAL-INFARCTION-1 Copy FinalDocument4 pagesMYOCARDIAL-INFARCTION-1 Copy FinalReizel GaasPas encore d'évaluation
- Diabetes Management.Document24 pagesDiabetes Management.Hasrul Muslih0% (1)
- Ijem 16 722Document11 pagesIjem 16 722TinaPas encore d'évaluation
- HipoglikemiaDocument7 pagesHipoglikemiakarisaPas encore d'évaluation
- Refeeding Syndrome PDFDocument5 pagesRefeeding Syndrome PDFManuel ArenasPas encore d'évaluation
- Ketogenic Diet and EpilepsyDocument13 pagesKetogenic Diet and EpilepsyDra Jessica Johanna GabaPas encore d'évaluation
- Hypoglycemia in Adults Clinical Manifestations, Definition, and CausesDocument1 pageHypoglycemia in Adults Clinical Manifestations, Definition, and CausesnovaPas encore d'évaluation
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionD'EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionPas encore d'évaluation
- Anesthesia For The Older PatientsDocument40 pagesAnesthesia For The Older PatientsRAHUL SUTHARPas encore d'évaluation
- Pacemakers & Implantable Cardioverter-Defibrillators (Icds) - Anaesthesia Tutorial of The Week 299 25 November 2013Document8 pagesPacemakers & Implantable Cardioverter-Defibrillators (Icds) - Anaesthesia Tutorial of The Week 299 25 November 2013Anup SasalattiPas encore d'évaluation
- 5 EkgDocument6 pages5 EkgJessica BPas encore d'évaluation
- Amniotic Fluid EmbolismDocument8 pagesAmniotic Fluid EmbolismjPas encore d'évaluation
- CHFDocument10 pagesCHFPowpOw SangalangPas encore d'évaluation
- Therapeutic Index 18 October 2005Document16 pagesTherapeutic Index 18 October 2005Tabitha JordanPas encore d'évaluation
- Goal: To Describe The Structure and Function of The Muscular SystemDocument24 pagesGoal: To Describe The Structure and Function of The Muscular SystemLayne Fuentes Padillo-Mapiguid100% (1)
- Cardiac Cycle CircusDocument6 pagesCardiac Cycle CircusShilpa RKPas encore d'évaluation
- Duran, Kayllien - Group 7 Sec ADocument5 pagesDuran, Kayllien - Group 7 Sec AKAYLLIEN DURANPas encore d'évaluation
- Thyroid Mark StarrDocument4 pagesThyroid Mark Starrveneet1812Pas encore d'évaluation
- KARDEKDocument44 pagesKARDEKyayanPas encore d'évaluation
- Termodiluicao PulmonarDocument7 pagesTermodiluicao PulmonarKarina ResendePas encore d'évaluation
- Chest To Abdomen AssessmentDocument16 pagesChest To Abdomen AssessmentLuzel Lapuz100% (1)
- Cardiac Dysfunction in Neurocritical Care An Autonomic PerspectiveDocument14 pagesCardiac Dysfunction in Neurocritical Care An Autonomic PerspectiveMELVIN BURTONPas encore d'évaluation
- MCQ Kardiorespirasi 16Document10 pagesMCQ Kardiorespirasi 16RevikaPas encore d'évaluation
- BioFluid Dynamics, Theory and ApprochDocument517 pagesBioFluid Dynamics, Theory and ApprochAshish Kotwal0% (1)
- Unit 1: Patient AdmissionsDocument10 pagesUnit 1: Patient AdmissionsSETIATY PANDIAPas encore d'évaluation
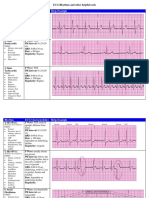
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasPas encore d'évaluation
- Human Body - 1Document9 pagesHuman Body - 1gemini_157Pas encore d'évaluation
- Basic Life SupportDocument6 pagesBasic Life SupportRyan Mathew ScottPas encore d'évaluation
- General Patho Lab2 2Document93 pagesGeneral Patho Lab2 2عبد الرحمن عصام ابوديابPas encore d'évaluation
- Management Functions - 1, PLANNING (Pls Check SyllabusDocument5 pagesManagement Functions - 1, PLANNING (Pls Check Syllabuslhara vhaneza cuetoPas encore d'évaluation
- Spot Diagnosis Using Pulse Wave Doppler Interrogation of The Abdominal AortaDocument2 pagesSpot Diagnosis Using Pulse Wave Doppler Interrogation of The Abdominal AortaHand SanitizerPas encore d'évaluation
- Kidney Transplant CriteriaDocument7 pagesKidney Transplant Criteriaapi-340699040Pas encore d'évaluation
- Elevate Your Client Sessions With Cellular Resonance® Quantum HealingDocument41 pagesElevate Your Client Sessions With Cellular Resonance® Quantum HealingStephen James100% (1)
- 3rd Year Cardio Lesson Plan 1Document139 pages3rd Year Cardio Lesson Plan 1Jeffery Samuel100% (1)
- (Uace) Abe Holy Cross LV Jinja 07th 10 2023Document20 pages(Uace) Abe Holy Cross LV Jinja 07th 10 2023bridgous3Pas encore d'évaluation