Vous aimerez peut-être aussi
- Displasias Verticais: Tratamento e Estabilidade da Mordida Aberta AnteriorDocument29 pagesDisplasias Verticais: Tratamento e Estabilidade da Mordida Aberta AnteriormutansPas encore d'évaluation
- Bionator UFSC: Protocolo de TratamentoDocument67 pagesBionator UFSC: Protocolo de Tratamentomutans100% (3)
- Bionator UFSC: Protocolo de TratamentoDocument67 pagesBionator UFSC: Protocolo de Tratamentomutans100% (3)
- Mesialização Com CursorDocument5 pagesMesialização Com CursormutansPas encore d'évaluation
- Plano de Educação Ambiental para Trabalhadores - Rev01Document7 pagesPlano de Educação Ambiental para Trabalhadores - Rev01smsengemon jequiePas encore d'évaluation
- Colagem de Bráquetes em Ortodontia: Uma RevisãoDocument12 pagesColagem de Bráquetes em Ortodontia: Uma RevisãomutansPas encore d'évaluation
- Receção de HotelDocument117 pagesReceção de HotelBrielSilcaPas encore d'évaluation
- Crescimento e desenvolvimento da maxilaDocument5 pagesCrescimento e desenvolvimento da maxilamutansPas encore d'évaluation
- Crescimento e desenvolvimento da maxilaDocument5 pagesCrescimento e desenvolvimento da maxilamutansPas encore d'évaluation
- A Vida de Uma Princesa Árabe Revela a Opressão das MulheresDocument144 pagesA Vida de Uma Princesa Árabe Revela a Opressão das MulheresMarcos Bezerra da CostaPas encore d'évaluation
- As Bases Das Relacoes SaudaveisDocument5 pagesAs Bases Das Relacoes Saudaveisfassisbr6137Pas encore d'évaluation
- Densidade de materiaisDocument2 pagesDensidade de materiaisPaulo Viegas0% (1)
- Correção de Mordida Profunda Com AlinhadoresDocument9 pagesCorreção de Mordida Profunda Com AlinhadoresmutansPas encore d'évaluation
- Micro ME850Document55 pagesMicro ME850api-3765629100% (1)
- Bionator X DTMDocument5 pagesBionator X DTMmutansPas encore d'évaluation
- Principais técnicas de controle de comportamento em OdontopediatriaDocument6 pagesPrincipais técnicas de controle de comportamento em OdontopediatriamutansPas encore d'évaluation
- BandagemDocument6 pagesBandagemmutansPas encore d'évaluation
- Efeitos do AEB e Bionator no tratamento da Classe IIDocument18 pagesEfeitos do AEB e Bionator no tratamento da Classe IImutansPas encore d'évaluation
- BandõesDocument5 pagesBandõescachorro996Pas encore d'évaluation
- Cap - 01 Crscimento CranioDocument12 pagesCap - 01 Crscimento CranioAnonymous 1lSXdhRBZ9Pas encore d'évaluation
- BionatorDocument7 pagesBionatorMaRii ALePas encore d'évaluation
- Quadri HeliceDocument12 pagesQuadri HeliceMartin AdriazolaPas encore d'évaluation
- Bionator - Protocolo Clínico (Mono)Document10 pagesBionator - Protocolo Clínico (Mono)mutansPas encore d'évaluation
- DTM e A Relação Com A Oclusão e A OrtodontiaDocument4 pagesDTM e A Relação Com A Oclusão e A OrtodontiamutansPas encore d'évaluation
- Cap 24 (ABO) Disfunções Temporo-Mandibulares em Bebês-Crianças-e-AdolescentesDocument11 pagesCap 24 (ABO) Disfunções Temporo-Mandibulares em Bebês-Crianças-e-AdolescentesmutansPas encore d'évaluation
- Amalgamas y Resinas en El Sector PosteriorDocument8 pagesAmalgamas y Resinas en El Sector PosteriormutansPas encore d'évaluation
- Radiog Panoramica e Odontop PDFDocument10 pagesRadiog Panoramica e Odontop PDFmutansPas encore d'évaluation
- Higiene bucal UTI pré-altaDocument4 pagesHigiene bucal UTI pré-altamutans100% (1)
- Amalgamas y Resinas en El Sector PosteriorDocument8 pagesAmalgamas y Resinas en El Sector PosteriormutansPas encore d'évaluation
- Características da oclusão na dentadura decíduaDocument16 pagesCaracterísticas da oclusão na dentadura decíduamutansPas encore d'évaluation
- Introdução À Psicologia Pré-NatalDocument20 pagesIntrodução À Psicologia Pré-NatalmutansPas encore d'évaluation
- Efeito do tratamento térmico nos fios ortodônticos de aço inoxidávelDocument104 pagesEfeito do tratamento térmico nos fios ortodônticos de aço inoxidávelmutansPas encore d'évaluation
- Efeito do tratamento térmico nos fios ortodônticos de aço inoxidávelDocument104 pagesEfeito do tratamento térmico nos fios ortodônticos de aço inoxidávelmutansPas encore d'évaluation
- Freio Labial Maxilar PDFDocument9 pagesFreio Labial Maxilar PDFmutansPas encore d'évaluation
- Saúde Bucal e Sua Associação Com o Estado Nutricional PDFDocument6 pagesSaúde Bucal e Sua Associação Com o Estado Nutricional PDFmutansPas encore d'évaluation
- 3 ObjetivaDocument4 pages3 ObjetivaViviane Araujo50% (2)
- Procedimento Operacional Padrão: TituloDocument7 pagesProcedimento Operacional Padrão: TituloDeyvid OliveiraPas encore d'évaluation
- Estatuto do servidor DiademaDocument46 pagesEstatuto do servidor Diademajmaj jmajPas encore d'évaluation
- Procedimentos para ensaio de viga de concreto protendidaDocument66 pagesProcedimentos para ensaio de viga de concreto protendidaLucasPas encore d'évaluation
- Trabalho Completo Ev154 MD1 Sa136 Id4319112021235951Document20 pagesTrabalho Completo Ev154 MD1 Sa136 Id4319112021235951LEAFAR ZAIDPas encore d'évaluation
- Lista de verificação para inclusão de arma por compra na indústria nacionalDocument1 pageLista de verificação para inclusão de arma por compra na indústria nacionalNet WalkerPas encore d'évaluation
- Fibra Tipo 3Document5 pagesFibra Tipo 3Edimilson LanaPas encore d'évaluation
- Regulamenta acautelamento de material bélico SEAPDocument26 pagesRegulamenta acautelamento de material bélico SEAPfaelcassioPas encore d'évaluation
- CO MUELLER - Bomba KSB 050-032-250 - Folha de DadosDocument6 pagesCO MUELLER - Bomba KSB 050-032-250 - Folha de DadosmarceloPas encore d'évaluation
- Conceitualização Cognitiva: Pensamentos, Crenças e EstratégiasDocument5 pagesConceitualização Cognitiva: Pensamentos, Crenças e EstratégiasMauricio Marane0% (1)
- Sistema tratamento efluentes residência 4 pessoasDocument3 pagesSistema tratamento efluentes residência 4 pessoasweber100% (1)
- Ap3 Pesquisa Mercadologica Uninta - Passei DiretoDocument11 pagesAp3 Pesquisa Mercadologica Uninta - Passei DiretoFelipe LimaPas encore d'évaluation
- O banco mais vantajoso: a esmolaDocument65 pagesO banco mais vantajoso: a esmolaParistomas Reports CenterPas encore d'évaluation
- Portugal - Marcas de Contrast Aria e de ResponsabilidadeDocument3 pagesPortugal - Marcas de Contrast Aria e de ResponsabilidadeClara RamosPas encore d'évaluation
- Criar ConteúdoDocument62 pagesCriar ConteúdoDavidCamarinhaPas encore d'évaluation
- Síndrome do chicote: revisão sobre lesão por aceleração cervicalDocument5 pagesSíndrome do chicote: revisão sobre lesão por aceleração cervicalCatarina DiasPas encore d'évaluation
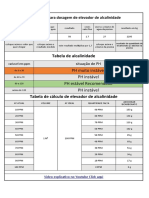
- Tabela de AlcalinidadeDocument1 pageTabela de AlcalinidadeedsonPas encore d'évaluation
- Proposta PME CPDocument8 pagesProposta PME CPlucas gameplayPas encore d'évaluation
- 2º Encontro Ciências 15-03-2022Document14 pages2º Encontro Ciências 15-03-2022Edson AraujoPas encore d'évaluation
- Orgânica3 Hidrocarbonetos (Parte1)Document21 pagesOrgânica3 Hidrocarbonetos (Parte1)Lorenzo RamosPas encore d'évaluation
- 2815-lms FileDocument5 pages2815-lms FileShayrula AlicePas encore d'évaluation
- SimposioANPEPP 2008Document178 pagesSimposioANPEPP 2008Hábilis Augusto BiazottoPas encore d'évaluation
- 878250-1 Lista de ExerciciosDocument2 pages878250-1 Lista de ExerciciosURANIOPas encore d'évaluation
- Inquerito - PFDocument10 pagesInquerito - PFliscappiPas encore d'évaluation
- Características à vazio e de curto-circuito de máquinas síncronasDocument6 pagesCaracterísticas à vazio e de curto-circuito de máquinas síncronasCláudia FonsecaPas encore d'évaluation