Vous aimerez peut-être aussi
- Dr. SANATH SHETTY - Philosophies of Full Mouth Rehab 4Document6 pagesDr. SANATH SHETTY - Philosophies of Full Mouth Rehab 4priya100% (2)
- Clinical Cases in Restorative and Reconstructive DentistryD'EverandClinical Cases in Restorative and Reconstructive DentistryÉvaluation : 5 sur 5 étoiles5/5 (1)
- Hobos PhilosophyDocument189 pagesHobos PhilosophysapnaPas encore d'évaluation
- Hobos PhilosophyDocument190 pagesHobos Philosophysapna100% (1)
- Pankey Mann Schuyler Technique of Oral RehabilitationDocument187 pagesPankey Mann Schuyler Technique of Oral RehabilitationAkanksha Mahajan50% (2)
- Prostho Vi - Slides 5 - Occlusal - ConsiderationsDocument83 pagesProstho Vi - Slides 5 - Occlusal - Considerationsبراءة أحمد السلاماتPas encore d'évaluation
- Occlusion Not ConfusionDocument13 pagesOcclusion Not ConfusionViorel IonPas encore d'évaluation
- Semcon3macaranasfinals 3Document19 pagesSemcon3macaranasfinals 3CT MacaranasPas encore d'évaluation
- Holistic Approach To Full Mouth Rehab PDFDocument5 pagesHolistic Approach To Full Mouth Rehab PDFAna AlvaradoPas encore d'évaluation
- Articulo Ajuste Oclusalu1994Document4 pagesArticulo Ajuste Oclusalu1994Marjorie Stefanie Rodriguez ReyesPas encore d'évaluation
- ACP, Ch7, Khalid AlshareefDocument7 pagesACP, Ch7, Khalid AlshareefKhalid Bin FaisalPas encore d'évaluation
- Occlusion in FPD and IMPLANTSDocument68 pagesOcclusion in FPD and IMPLANTSDRSH100% (1)
- F Methods of Recording Centric Relation FinalDocument17 pagesF Methods of Recording Centric Relation FinalJyoti TripathiPas encore d'évaluation
- Considerations When Planning Occlusal Rehabilitation: Review of The LiteratureDocument11 pagesConsiderations When Planning Occlusal Rehabilitation: Review of The LiteratureKathy Cuevas HinojosaPas encore d'évaluation
- Diagnostic Procedures and Articulation Occlusion 2021-2022Document43 pagesDiagnostic Procedures and Articulation Occlusion 2021-2022محمد ربيعيPas encore d'évaluation
- ORTHO Intercep. 25Document54 pagesORTHO Intercep. 25desktop dolakhaPas encore d'évaluation
- Full Mouth RehabDocument9 pagesFull Mouth RehabpragatiPas encore d'évaluation
- Oclusion in CD ProsthoDocument62 pagesOclusion in CD ProsthoFourthMolar.com50% (2)
- Hinge Axis and FacebowDocument80 pagesHinge Axis and FacebowDrSadaf KazmiPas encore d'évaluation
- !excellence in Finishing Current Concepts Goals and Mechanics PDFDocument13 pages!excellence in Finishing Current Concepts Goals and Mechanics PDFMargarita Lopez Martinez100% (1)
- Thin Book of OcclusionDocument7 pagesThin Book of OcclusionDavid LiPas encore d'évaluation
- The Major Part of Dentistry You May Be Neglecting: ObservationsDocument3 pagesThe Major Part of Dentistry You May Be Neglecting: ObservationsQuynh NguyenPas encore d'évaluation
- File Full 2731Document14 pagesFile Full 2731จิตติศักดิ์ สุวรรณPas encore d'évaluation
- Occlusion in Complete Denture Part IDocument34 pagesOcclusion in Complete Denture Part IهجرسPas encore d'évaluation
- Functional Appliance Selection Criteria - PraveenaDocument109 pagesFunctional Appliance Selection Criteria - PraveenaBimalKrishna50% (2)
- 7 - Occlusal Concepts For Complete Denture Occlusion1Document42 pages7 - Occlusal Concepts For Complete Denture Occlusion1Haytham EmadPas encore d'évaluation
- Occlusion For StabilityDocument8 pagesOcclusion For StabilitydrsmritiPas encore d'évaluation
- Oclusion OralDocument8 pagesOclusion OralzayraPas encore d'évaluation
- Balanced Occlusion: by Reema Talat Ayesha Final Year R.R.D.CDocument31 pagesBalanced Occlusion: by Reema Talat Ayesha Final Year R.R.D.CArunPas encore d'évaluation
- Incisor Alignment With The Inman Aligner: C S W & WDocument13 pagesIncisor Alignment With The Inman Aligner: C S W & WShaghayegh SahraPas encore d'évaluation
- Occlusion and Removable ProsthodonticsDocument8 pagesOcclusion and Removable ProsthodonticsMarylin AngPas encore d'évaluation
- The Influence of Anterior Coupling On Mandibular MovementDocument9 pagesThe Influence of Anterior Coupling On Mandibular MovementRavneet LehalPas encore d'évaluation
- Occlusal Schemes in FPDDocument6 pagesOcclusal Schemes in FPDPadmini ReddyPas encore d'évaluation
- Presented By-Anupriya Srivastava Mds III RD YearDocument93 pagesPresented By-Anupriya Srivastava Mds III RD YearParijat Chakraborty PJPas encore d'évaluation
- Occlusion in Partial Dentures: by Prof. Dr. Osama BarakaDocument12 pagesOcclusion in Partial Dentures: by Prof. Dr. Osama BarakaEsmail AhmedPas encore d'évaluation
- Occlusion in Fixed ProsthodonticsDocument14 pagesOcclusion in Fixed ProsthodonticsGayathri GangadharanPas encore d'évaluation
- Occlusion in Relation To Removable Partial DentureDocument15 pagesOcclusion in Relation To Removable Partial DentureVikas AggarwalPas encore d'évaluation
- Lec 8Document7 pagesLec 8Dr.Haider Saleem AbdullahPas encore d'évaluation
- Review Article in ProsthodonticsDocument8 pagesReview Article in ProsthodonticsChandrika VeerareddyPas encore d'évaluation
- GPT 9Document37 pagesGPT 9MohamedPas encore d'évaluation
- 7 Horizontal Jaw RelationsDocument11 pages7 Horizontal Jaw Relationsعلي محمود جمالPas encore d'évaluation
- Fundamentals For Orientation of Occlusal Plane inDocument4 pagesFundamentals For Orientation of Occlusal Plane innurqumirfanPas encore d'évaluation
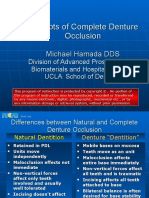
- Concepts of Complete Denture OcclusionDocument39 pagesConcepts of Complete Denture Occlusionaziz2007100% (1)
- Functional OcclusionDocument14 pagesFunctional OcclusionAbdul MohaiminPas encore d'évaluation
- Full Mouth Rehabilitation: Presented by DR - Namitha AP 3rd MDSDocument270 pagesFull Mouth Rehabilitation: Presented by DR - Namitha AP 3rd MDSAkanksha Mahajan100% (1)
- Schuyler1953 PDFDocument11 pagesSchuyler1953 PDFMayank MalraPas encore d'évaluation
- Review Article: Occlusal Schemes For Complete Dentures - A Review ArticleDocument6 pagesReview Article: Occlusal Schemes For Complete Dentures - A Review ArticleoktikikiPas encore d'évaluation
- Hassall 2021Document6 pagesHassall 2021DhanasriPas encore d'évaluation
- Hanashima Et Al. - 2009 - A Study Regarding Occlusal Plane and Posterior Disocclusion-AnnotatedDocument8 pagesHanashima Et Al. - 2009 - A Study Regarding Occlusal Plane and Posterior Disocclusion-AnnotatedJonathan GIraldo Martinez100% (1)
- ABO Grading SystemDocument82 pagesABO Grading Systemsanjeed sanjuPas encore d'évaluation
- Horizontal Jaw RelationDocument28 pagesHorizontal Jaw RelationVidya SenthuPas encore d'évaluation
- Dental ArticulatorsDocument10 pagesDental ArticulatorsOmar Al-FatyanPas encore d'évaluation
- 21twin BlockDocument106 pages21twin Blockshweta nagesh100% (1)
- How To Effectively Use A 264 Appliance: Features SectionDocument11 pagesHow To Effectively Use A 264 Appliance: Features Sectionvefiisphepy83312Pas encore d'évaluation
- Art 2Document6 pagesArt 2Joyce Stefania Posada MauricioPas encore d'évaluation
- Occlusal Concepts in Full Mouth Rehabilitation: An OverviewDocument8 pagesOcclusal Concepts in Full Mouth Rehabilitation: An OverviewShanna MitchellPas encore d'évaluation
- 4813305a PDFDocument6 pages4813305a PDFgattusoPas encore d'évaluation
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanPas encore d'évaluation
- كل أسئلة اللثة لامتحان الهيئةDocument40 pagesكل أسئلة اللثة لامتحان الهيئةMohamed Kudaih100% (1)
- KAUFD+Student+Handbook+2011 2012Document147 pagesKAUFD+Student+Handbook+2011 2012Mohamed KudaihPas encore d'évaluation
- Orca Share Media1470336125733Document103 pagesOrca Share Media1470336125733Fatima SiddiquiPas encore d'évaluation
- SLE 2015, Compilation of Test Questions: 8 5 5 M C Q SDocument99 pagesSLE 2015, Compilation of Test Questions: 8 5 5 M C Q SAbdelreheem ElgendyPas encore d'évaluation
- Sle Final JuneDocument40 pagesSle Final JuneMohamed KudaihPas encore d'évaluation
- Ahmed SLE Mcq-P2 - E2 - 80 - AB - E2 - 80 - AC PDFDocument172 pagesAhmed SLE Mcq-P2 - E2 - 80 - AB - E2 - 80 - AC PDFMohamed Kudaih100% (4)
- Sle Final JuneDocument40 pagesSle Final JuneMohamed KudaihPas encore d'évaluation
- كل أسئلة اللثة لامتحان الهيئةDocument41 pagesكل أسئلة اللثة لامتحان الهيئةMohamed KudaihPas encore d'évaluation
- ImplantDocument4 pagesImplantMohamed KudaihPas encore d'évaluation
- Sat 2Document1 pageSat 2Mohamed KudaihPas encore d'évaluation
- Please Subscribe To My ChannelDocument1 pagePlease Subscribe To My ChannelMohamed KudaihPas encore d'évaluation
- Nejmoa2107038 AppendixDocument38 pagesNejmoa2107038 Appendixsri wahyuniPas encore d'évaluation
- 2016 S 0042 108641 PDFDocument29 pages2016 S 0042 108641 PDFMadalina StoicescuPas encore d'évaluation
- Mnemonics ShortDocument139 pagesMnemonics ShortKelly HernandezPas encore d'évaluation
- BLS Interim Material 2020 - Provider Manual ChangesDocument2 pagesBLS Interim Material 2020 - Provider Manual ChangesyossyusPas encore d'évaluation
- Acne Vulgaris DiscussionDocument46 pagesAcne Vulgaris Discussiondrsaleemraza2004Pas encore d'évaluation
- Deped Copy: Unit 1: Consumer HealthDocument34 pagesDeped Copy: Unit 1: Consumer HealthMelody Derapite LandichoPas encore d'évaluation
- Cerebral Palsy CaseDocument13 pagesCerebral Palsy CaseAnusree AnusreervPas encore d'évaluation
- Tugas Mencari LiteraturDocument140 pagesTugas Mencari LiteraturKoko WicaksonoPas encore d'évaluation
- Airway-RSI Pocket CardDocument4 pagesAirway-RSI Pocket CardbellerevoltePas encore d'évaluation
- MonevaDocument7 pagesMonevamadhellePas encore d'évaluation
- Absite Questions MissedDocument11 pagesAbsite Questions Misseddrmdz3Pas encore d'évaluation
- Journal ClubDocument19 pagesJournal ClubHemshree ParmarPas encore d'évaluation
- MDS (Periodontology) : Applied Anatomy, Physiology, Biochemistry, Pathology and PharmacologyDocument4 pagesMDS (Periodontology) : Applied Anatomy, Physiology, Biochemistry, Pathology and Pharmacologydeepak sharmaPas encore d'évaluation
- Herniated Nucleus Pulposus in Dr. Hasan Sadikin General Hospital Bandung IndonesiaDocument7 pagesHerniated Nucleus Pulposus in Dr. Hasan Sadikin General Hospital Bandung Indonesiawulan dwi yulistiaPas encore d'évaluation
- Erb's PalsyDocument18 pagesErb's PalsyMegha PataniPas encore d'évaluation
- Assessment of Foot PostureDocument3 pagesAssessment of Foot Posturejona_kinePas encore d'évaluation
- FK Conox Product Brochure 4ppa4 v6Document4 pagesFK Conox Product Brochure 4ppa4 v6Lucas ShotsPas encore d'évaluation
- Quality Management-Mabruri JurnalisDocument18 pagesQuality Management-Mabruri JurnalisMabrury JurnalisPas encore d'évaluation
- OHQoL. - LEA KRAGT de Ross PDFDocument218 pagesOHQoL. - LEA KRAGT de Ross PDFancaPas encore d'évaluation
- Emily Costello Pharmd CVDocument5 pagesEmily Costello Pharmd CVapi-715270205Pas encore d'évaluation
- Who Classification of Head & Neck Tumors - 2017Document343 pagesWho Classification of Head & Neck Tumors - 2017Pablo Enrique Mejia Paz78% (40)
- Curriculum Vitae - Sopiyudin Dahlan (03!23!17!01!01-08)Document8 pagesCurriculum Vitae - Sopiyudin Dahlan (03!23!17!01!01-08)Eva ArdiantiPas encore d'évaluation
- Androgenetic Alopecia and Coronary Artery Disease CASE CONTROL STUDY DR RAHUL KUMAR SHARMA SKIN SPECIALIST AJMERDocument2 pagesAndrogenetic Alopecia and Coronary Artery Disease CASE CONTROL STUDY DR RAHUL KUMAR SHARMA SKIN SPECIALIST AJMERRahul SharmaPas encore d'évaluation
- Minimental ParkinsonDocument9 pagesMinimental ParkinsondquebradasPas encore d'évaluation
- Children's Community Nursing: Promoting Effective Teamworking For Children and Their FamiliesDocument26 pagesChildren's Community Nursing: Promoting Effective Teamworking For Children and Their FamiliesRaiHanah HasanPas encore d'évaluation
- Operative Vaginal Delivery PDFDocument56 pagesOperative Vaginal Delivery PDFFarehan Md IsaPas encore d'évaluation
- NCP NewbornDocument8 pagesNCP Newbornsupacalifragirlistic67% (9)
- Pulmonary EdemaDocument28 pagesPulmonary EdemaMohammed Elias100% (1)
- IMF Screw Set. For Temporary, Peri Operative Stabilisation of The Occlusion in AdultsDocument12 pagesIMF Screw Set. For Temporary, Peri Operative Stabilisation of The Occlusion in AdultsAnonymous LnWIBo1GPas encore d'évaluation
- Pediatric DehydrationDocument27 pagesPediatric DehydrationAbraham ChiuPas encore d'évaluation
- FreeCAD | Step by Step: Learn how to easily create 3D objects, assemblies, and technical drawingsD'EverandFreeCAD | Step by Step: Learn how to easily create 3D objects, assemblies, and technical drawingsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Autodesk Inventor 2020: A Power Guide for Beginners and Intermediate UsersD'EverandAutodesk Inventor 2020: A Power Guide for Beginners and Intermediate UsersPas encore d'évaluation
- CATIA V5-6R2015 Basics - Part I : Getting Started and Sketcher WorkbenchD'EverandCATIA V5-6R2015 Basics - Part I : Getting Started and Sketcher WorkbenchÉvaluation : 4 sur 5 étoiles4/5 (10)
- Beginning AutoCAD® 2020 Exercise WorkbookD'EverandBeginning AutoCAD® 2020 Exercise WorkbookÉvaluation : 2.5 sur 5 étoiles2.5/5 (3)
- SketchUp Success for Woodworkers: Four Simple Rules to Create 3D Drawings Quickly and AccuratelyD'EverandSketchUp Success for Woodworkers: Four Simple Rules to Create 3D Drawings Quickly and AccuratelyÉvaluation : 1.5 sur 5 étoiles1.5/5 (2)
- Product Manufacturing and Cost Estimating using CAD/CAE: The Computer Aided Engineering Design SeriesD'EverandProduct Manufacturing and Cost Estimating using CAD/CAE: The Computer Aided Engineering Design SeriesÉvaluation : 4 sur 5 étoiles4/5 (4)
- Autodesk Fusion 360: A Power Guide for Beginners and Intermediate Users (3rd Edition)D'EverandAutodesk Fusion 360: A Power Guide for Beginners and Intermediate Users (3rd Edition)Évaluation : 5 sur 5 étoiles5/5 (2)
- Certified Solidworks Professional Advanced Weldments Exam PreparationD'EverandCertified Solidworks Professional Advanced Weldments Exam PreparationÉvaluation : 5 sur 5 étoiles5/5 (1)
- Beginning AutoCAD® 2022 Exercise Workbook: For Windows®D'EverandBeginning AutoCAD® 2022 Exercise Workbook: For Windows®Pas encore d'évaluation
- Certified Solidworks Professional Advanced Surface Modeling Exam PreparationD'EverandCertified Solidworks Professional Advanced Surface Modeling Exam PreparationÉvaluation : 5 sur 5 étoiles5/5 (1)
- 2024 – 2025 Newbies Guide to UI/UX Design Using FigmaD'Everand2024 – 2025 Newbies Guide to UI/UX Design Using FigmaPas encore d'évaluation
- Up and Running with AutoCAD 2020: 2D Drafting and DesignD'EverandUp and Running with AutoCAD 2020: 2D Drafting and DesignPas encore d'évaluation
- FreeCAD | Design Projects: Design advanced CAD models step by stepD'EverandFreeCAD | Design Projects: Design advanced CAD models step by stepÉvaluation : 5 sur 5 étoiles5/5 (1)
- Contactless Vital Signs MonitoringD'EverandContactless Vital Signs MonitoringWenjin WangPas encore d'évaluation