Vous aimerez peut-être aussi
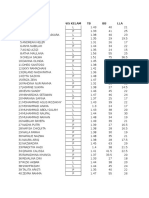
- Data Antro SDNP1-Peb 2017Document11 pagesData Antro SDNP1-Peb 2017mantabsipPas encore d'évaluation
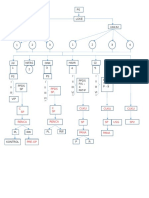
- Alur IcaDocument1 pageAlur IcamantabsipPas encore d'évaluation
- Kuliah Blok Bleeding DisordersDocument39 pagesKuliah Blok Bleeding DisordersmantabsipPas encore d'évaluation
- Bleeding Disorders VKDBDocument30 pagesBleeding Disorders VKDBmantabsipPas encore d'évaluation
- Overview DeathcaseDocument4 pagesOverview DeathcasemantabsipPas encore d'évaluation
- Blok 2-Bioscience Schedule DD IKA2Document1 pageBlok 2-Bioscience Schedule DD IKA2mantabsipPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Test Bank For Introduction To Critical Care Nursing 5th Edition Mary Lou SoleDocument9 pagesTest Bank For Introduction To Critical Care Nursing 5th Edition Mary Lou Solemammonphysics2e1.w4Pas encore d'évaluation
- Report - For MaamDocument7 pagesReport - For MaamSherchen Antonio-CortesPas encore d'évaluation
- Sean Benesh Cover Letter 10-1-23Document1 pageSean Benesh Cover Letter 10-1-23api-708800698Pas encore d'évaluation
- Endodontic Clinic Manual 2015 - 1Document134 pagesEndodontic Clinic Manual 2015 - 1Adina Popa100% (2)
- Gale Global PPNU 2019-11-01Document410 pagesGale Global PPNU 2019-11-01s4sigitPas encore d'évaluation
- FAQs KCRKITDocument2 pagesFAQs KCRKITRohith RohanPas encore d'évaluation
- Medicalization: History and Theory HSSC 532 /HIST 534/SOCI 513Document4 pagesMedicalization: History and Theory HSSC 532 /HIST 534/SOCI 513sofroniscoPas encore d'évaluation
- Maternity Pediatric Nursing 3rd Ricci Test BankDocument8 pagesMaternity Pediatric Nursing 3rd Ricci Test Banksonyaaaq0% (1)
- V-Moringa LinimentDocument1 pageV-Moringa LinimentJeremy Tausa-alexopoulosPas encore d'évaluation
- Medical Helminthology Introduction PDFDocument13 pagesMedical Helminthology Introduction PDFfaiz0% (1)
- ESI Hospital BhubaneswarDocument3 pagesESI Hospital BhubaneswarsureesicPas encore d'évaluation
- Salter, J. (2014) - Behind The Screen. Demos, London.Document122 pagesSalter, J. (2014) - Behind The Screen. Demos, London.brenderdanPas encore d'évaluation
- NCP PretermDocument5 pagesNCP PretermJamine Joyce Ortega-AlvarezPas encore d'évaluation
- Section 9 - Students WorksheetDocument6 pagesSection 9 - Students WorksheetEsraa AhmedPas encore d'évaluation
- Pancreatic Cancer - Yesterday, Today and Tomorrow PDFDocument18 pagesPancreatic Cancer - Yesterday, Today and Tomorrow PDFAndrei TatomirPas encore d'évaluation
- ARBOVIRUS 2014 PriyoDocument38 pagesARBOVIRUS 2014 PriyoPaskalia NikenPas encore d'évaluation
- Jenny E. Pennycuff, M.D., M.S.: Present PositionDocument10 pagesJenny E. Pennycuff, M.D., M.S.: Present Positionapi-625759582Pas encore d'évaluation
- Schistosomiasis: Caused by Blood Flukes (Trematode Worms) of The Genus SchistosomaDocument2 pagesSchistosomiasis: Caused by Blood Flukes (Trematode Worms) of The Genus SchistosomakyawPas encore d'évaluation
- Apical Patency - ARTICULO 2Document4 pagesApical Patency - ARTICULO 2Karina Delgado MejíaPas encore d'évaluation
- Claim Process PDFDocument16 pagesClaim Process PDFsknrPas encore d'évaluation
- Iio Ow Waa B Bo Oaarrd D O Off N Nu Urrssiin NG GDocument34 pagesIio Ow Waa B Bo Oaarrd D O Off N Nu Urrssiin NG GWichipirichiPas encore d'évaluation
- Introduction, History, Scope, Routes of Drug AdministrationDocument49 pagesIntroduction, History, Scope, Routes of Drug AdministrationNoor VirkPas encore d'évaluation
- Maggot Therapy For Treating Diabetic Foot Ulcers UDocument6 pagesMaggot Therapy For Treating Diabetic Foot Ulcers UBayu AdhityaPas encore d'évaluation
- Hahnemann S., Chronic DisDocument167 pagesHahnemann S., Chronic Dishompat100% (1)
- Human Papillomavirus InfectionDocument78 pagesHuman Papillomavirus InfectionJoaquín PeñaPas encore d'évaluation
- 6 Minute Walk Test ATS GuidelinesDocument7 pages6 Minute Walk Test ATS GuidelinescpradheepPas encore d'évaluation
- Sources of Drug InformationDocument36 pagesSources of Drug InformationCristine ChubiboPas encore d'évaluation
- AbortionDocument35 pagesAbortionHoney May Rollan VicentePas encore d'évaluation
- CPCR NewDocument30 pagesCPCR NewPhil PhilipsPas encore d'évaluation
- Mifepristone & Misoprostol Dosing Chart 2023Document1 pageMifepristone & Misoprostol Dosing Chart 2023Iriawan Indra PutraPas encore d'évaluation