Vous aimerez peut-être aussi
- Bang Hendi 3Document10 pagesBang Hendi 3Jacky JunaediPas encore d'évaluation
- TegarDOPS DR LusitoDocument3 pagesTegarDOPS DR LusitoImada KhoironiPas encore d'évaluation
- Jurnal InternaDocument6 pagesJurnal InternaImada KhoironiPas encore d'évaluation
- Laily Lbm5 THT - Painful SwallowingDocument30 pagesLaily Lbm5 THT - Painful SwallowingImada KhoironiPas encore d'évaluation
- Coffee Consumption and Risk of Hypertension in The Polish Arm of The HAPIEE Cohort StudyDocument7 pagesCoffee Consumption and Risk of Hypertension in The Polish Arm of The HAPIEE Cohort StudyImada KhoironiPas encore d'évaluation
- DsgesrtnjtrmntyjyuDocument1 pageDsgesrtnjtrmntyjyuImada KhoironiPas encore d'évaluation
- CXR FundamentalDocument43 pagesCXR FundamentalImada KhoironiPas encore d'évaluation
- Resuscitation Fluids - NEJMDocument9 pagesResuscitation Fluids - NEJMJHWPas encore d'évaluation
- Paraumbilical Umbilical HerniaDocument4 pagesParaumbilical Umbilical HerniaImada KhoironiPas encore d'évaluation
- Laily Lbm5 THT - Painful SwallowingDocument30 pagesLaily Lbm5 THT - Painful SwallowingImada KhoironiPas encore d'évaluation
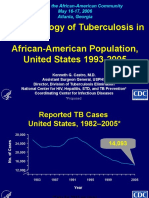
- Epidemiology of Tuberculosis in African-American Population, United States 1993-2005Document20 pagesEpidemiology of Tuberculosis in African-American Population, United States 1993-2005Imada KhoironiPas encore d'évaluation
- TB TreatDocument5 pagesTB Treatluvly_nara2802Pas encore d'évaluation
- Demam Tifoid Dr-IdaDocument45 pagesDemam Tifoid Dr-IdaJoseph WilsonPas encore d'évaluation
- CXR FundamentalDocument43 pagesCXR FundamentalImada KhoironiPas encore d'évaluation
- PEMERIKSAAN THORAX AND JANTUNGDocument59 pagesPEMERIKSAAN THORAX AND JANTUNGImada KhoironiPas encore d'évaluation
- LI LBM 2 Modul 5 - Hana Nisrina AlmasDocument12 pagesLI LBM 2 Modul 5 - Hana Nisrina AlmasImada KhoironiPas encore d'évaluation
- Journal Reading: Resuscitation FluidsDocument26 pagesJournal Reading: Resuscitation FluidsKikyPas encore d'évaluation
- Kuliah SKADocument34 pagesKuliah SKAHabibah Nurla LumierePas encore d'évaluation
- 2964 CONSORT+2010+ChecklistDocument3 pages2964 CONSORT+2010+ChecklistNur UlayatilmiladiyyahPas encore d'évaluation
- CPR & Electrical TherapiesDocument67 pagesCPR & Electrical TherapiesRizaldy Yoga67% (3)
- 2964 CONSORT+2010+ChecklistDocument3 pages2964 CONSORT+2010+ChecklistNur UlayatilmiladiyyahPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- 4MB0 02R Que 20160609 PDFDocument32 pages4MB0 02R Que 20160609 PDFakashPas encore d'évaluation
- Ragavendhar Seeks Entry Software JobDocument2 pagesRagavendhar Seeks Entry Software JobfferferfPas encore d'évaluation
- Basic Concepts of Citrix XenAppDocument13 pagesBasic Concepts of Citrix XenAppAvinash KumarPas encore d'évaluation
- Thank you for purchasing your remap from HDI Tuning LtdDocument2 pagesThank you for purchasing your remap from HDI Tuning LtdMaks LebanPas encore d'évaluation
- Makerwys - Exe Version 4.891: by Pete Dowson © 2019 InstructionsDocument11 pagesMakerwys - Exe Version 4.891: by Pete Dowson © 2019 InstructionsRafrol RamonPas encore d'évaluation
- Readme cljM880fw 2305076 518488 PDFDocument37 pagesReadme cljM880fw 2305076 518488 PDFjuan carlos MalagonPas encore d'évaluation
- Haier's Performance Management in Other CulturesDocument8 pagesHaier's Performance Management in Other CulturesSubhransu SahooPas encore d'évaluation
- Chime Primary School Brochure TemplateDocument1 pageChime Primary School Brochure TemplateNita HanifahPas encore d'évaluation
- Money MBA 1Document4 pagesMoney MBA 1neaman_ahmed0% (1)
- LaQshya Labour Room Quality Improvement InitiativeDocument2 pagesLaQshya Labour Room Quality Improvement InitiativeHimanshu SharmaPas encore d'évaluation
- EPM Mid Lecture 03 Chapt 1Document17 pagesEPM Mid Lecture 03 Chapt 1Partho Protim MondolPas encore d'évaluation
- Prperman 2016 14 3 (Spec. 14Document8 pagesPrperman 2016 14 3 (Spec. 14celia rifaPas encore d'évaluation
- Key Elements of Participation and Conflict Resolution in a DemocracyDocument6 pagesKey Elements of Participation and Conflict Resolution in a DemocracyAbhinayPas encore d'évaluation
- Literature Revisited: Understanding Key Concepts and Applying Analytical SkillsDocument31 pagesLiterature Revisited: Understanding Key Concepts and Applying Analytical SkillsMuhammad Furqan Aslam Awan100% (2)
- JKR Specs L-S1 Addendum No 1 LED Luminaires - May 2011Document3 pagesJKR Specs L-S1 Addendum No 1 LED Luminaires - May 2011Leong KmPas encore d'évaluation
- MEC332-MA 3rd Sem - Development EconomicsDocument9 pagesMEC332-MA 3rd Sem - Development EconomicsRITUPARNA KASHYAP 2239239Pas encore d'évaluation
- Sample ResumeDocument3 pagesSample Resumeapi-380209683% (6)
- Balzac and the Little Chinese Seamstress: A Journey During the Cultural RevolutionDocument4 pagesBalzac and the Little Chinese Seamstress: A Journey During the Cultural RevolutionRogona 123Pas encore d'évaluation
- Eports: India's Defiance of Religious Freedom: A Briefing On Anti-Conversion' LawsDocument16 pagesEports: India's Defiance of Religious Freedom: A Briefing On Anti-Conversion' LawsGabriela StevensPas encore d'évaluation
- STR File Varun 3Document61 pagesSTR File Varun 3Varun mendirattaPas encore d'évaluation
- Solwezi General Mental Health TeamDocument35 pagesSolwezi General Mental Health TeamHumphreyPas encore d'évaluation
- Article 106899Document6 pagesArticle 106899Abhinave SPas encore d'évaluation
- ccpc15 Supportive and Preventive WorkbookDocument30 pagesccpc15 Supportive and Preventive WorkbookJeremy HamptonPas encore d'évaluation
- DelhiDocument40 pagesDelhiRahul DharPas encore d'évaluation
- Cls A310 Operations ManualDocument23 pagesCls A310 Operations ManualAntonio Ahijado Mendieta100% (2)
- Catalogue MinicenterDocument36 pagesCatalogue Minicentermohamed mahdiPas encore d'évaluation
- Finding My Voice in ChinatownDocument5 pagesFinding My Voice in ChinatownMagalí MainumbyPas encore d'évaluation
- Njhs Application EssayDocument4 pagesNjhs Application Essaycjawrknbf100% (2)
- A Laboratory Experiment in Crystals and Crystal Model Building ObjectivesDocument7 pagesA Laboratory Experiment in Crystals and Crystal Model Building ObjectivesrajaaPas encore d'évaluation
- Balajit Nath Pandita-Specific Principles of Kashmir Saivism-Munshiram Manoharlal Publishers (1998) PDFDocument228 pagesBalajit Nath Pandita-Specific Principles of Kashmir Saivism-Munshiram Manoharlal Publishers (1998) PDFvramaniitkPas encore d'évaluation