Vous aimerez peut-être aussi
- Motor DB58TIS PDFDocument198 pagesMotor DB58TIS PDFRonaldi motter75% (16)
- D4607 1378898 1 Standard Test Method For Determination of Iodine Number of Activated Carbon PDFDocument5 pagesD4607 1378898 1 Standard Test Method For Determination of Iodine Number of Activated Carbon PDFMuthu KumarPas encore d'évaluation
- Antihypertensive DrugsDocument2 pagesAntihypertensive DrugsJillary LlagunoPas encore d'évaluation
- Risk Assesment Form - Ball MillingDocument6 pagesRisk Assesment Form - Ball Millingbc150Pas encore d'évaluation
- Asthma DrugsDocument1 pageAsthma DrugskakuPas encore d'évaluation
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDocument2 pagesDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariPas encore d'évaluation
- Pain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Document3 pagesPain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Ryan TurnerPas encore d'évaluation
- Antiepileptic DrugsDocument65 pagesAntiepileptic DrugsZarish IftikharPas encore d'évaluation
- Drugs For Diabetes MellitusDocument3 pagesDrugs For Diabetes MellitusGerardLum100% (1)
- 3-Major Veins of The BodyDocument26 pages3-Major Veins of The BodyTJPlayz100% (1)
- Drug Therapy of EpilepsiesDocument43 pagesDrug Therapy of EpilepsiesZobayer Ahmed100% (1)
- All Objectives HematologyDocument45 pagesAll Objectives HematologyNursing200980% (5)
- Antihypertensive AgentsDocument2 pagesAntihypertensive Agentskryscae nacarPas encore d'évaluation
- Drugs For AsthmaDocument3 pagesDrugs For AsthmaMelissa Deso MillerPas encore d'évaluation
- LesionsDocument16 pagesLesionsKevin NelsonPas encore d'évaluation
- Asthma Drugs Clinical PharmacologyDocument3 pagesAsthma Drugs Clinical PharmacologycrystalshePas encore d'évaluation
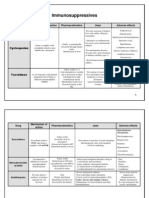
- 1 - Immuno Tables1Document4 pages1 - Immuno Tables1Urugonda VenumadhavPas encore d'évaluation
- Drug Moa PK Use Se Ci Blood Coagulation: AnticoagulantsDocument4 pagesDrug Moa PK Use Se Ci Blood Coagulation: AnticoagulantsYusoff RamdzanPas encore d'évaluation
- Cvs (Diuretics)Document2 pagesCvs (Diuretics)CatPas encore d'évaluation
- Anti Viral DrugsDocument6 pagesAnti Viral DrugskakuPas encore d'évaluation
- AlcoholsDocument23 pagesAlcoholsdhaineyPas encore d'évaluation
- ANS PharmacologyDocument58 pagesANS Pharmacologyalemu100% (1)
- Drug ClassDocument13 pagesDrug ClassEdfren Salazar Colon100% (1)
- Homeostatic Function of Thyroid and Parathyroid Gland & Calcium HomeostasisDocument15 pagesHomeostatic Function of Thyroid and Parathyroid Gland & Calcium HomeostasisGEETA MOHANPas encore d'évaluation
- Immune System Docs 2019Document13 pagesImmune System Docs 2019David DavidPas encore d'évaluation
- Hematologic DisordersDocument32 pagesHematologic DisordersQuolette ConstantePas encore d'évaluation
- Analgesic OintmentDocument1 pageAnalgesic OintmentLorenPas encore d'évaluation
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KPas encore d'évaluation
- Chapter 29Document3 pagesChapter 29monster40lbs100% (1)
- Morphine (Astramorph)Document1 pageMorphine (Astramorph)Adrianne BazoPas encore d'évaluation
- Anti Hypertensive Drugs - ACE InhibitorDocument16 pagesAnti Hypertensive Drugs - ACE InhibitorApurba Sarker Apu100% (1)
- Beta-Lactam Antibiotics & Other Cell Wall Synthesis InhibitorsDocument29 pagesBeta-Lactam Antibiotics & Other Cell Wall Synthesis InhibitorsRen PastelPas encore d'évaluation
- Benedict - S Test - FinalDocument28 pagesBenedict - S Test - FinalTom Anthony TonguiaPas encore d'évaluation
- Alpha BlockersDocument17 pagesAlpha BlockersKashis SharmaPas encore d'évaluation
- Baby Katzung Case 1 10Document15 pagesBaby Katzung Case 1 10Danielle Sabrina LimPas encore d'évaluation
- Cholinergic Pharmacology - Drug TableDocument2 pagesCholinergic Pharmacology - Drug TableFPas encore d'évaluation
- Study Guide Hematologic AssessmentDocument5 pagesStudy Guide Hematologic AssessmentNancy LemusPas encore d'évaluation
- NSAIDS and SteroidsDocument2 pagesNSAIDS and Steroidsmed testPas encore d'évaluation
- Master Pharm Drug ListDocument1 pageMaster Pharm Drug ListMichelle StramPas encore d'évaluation
- Physiology of The Special SensesDocument16 pagesPhysiology of The Special SensesRain Repas100% (1)
- Anaemia: What Is Anemia?Document21 pagesAnaemia: What Is Anemia?Rashed ShatnawiPas encore d'évaluation
- Approach To Unconscious PatientDocument23 pagesApproach To Unconscious Patienttantw880% (1)
- 1 6 Regulation of Blood Glucose PDFDocument3 pages1 6 Regulation of Blood Glucose PDFtiaraPas encore d'évaluation
- Basic Principles of PharmacologyDocument13 pagesBasic Principles of Pharmacologyemmanuel100% (1)
- (PHYSIO) 1.05 Autonomic Nervous System (EGBartolome)Document7 pages(PHYSIO) 1.05 Autonomic Nervous System (EGBartolome)Izza Mari DeLeon Laurio100% (2)
- AntiepilepticsDocument25 pagesAntiepilepticsMurali Krishna Kumar MuthyalaPas encore d'évaluation
- Revised Introduction To The Pharmacology of CNS DrugsDocument9 pagesRevised Introduction To The Pharmacology of CNS DrugsJoshua Ty CayetanoPas encore d'évaluation
- Pharmacology StudentnotesDocument55 pagesPharmacology StudentnotesPasalau Daria VasilicaPas encore d'évaluation
- Immune System Review QuestionsDocument2 pagesImmune System Review Questionsapi-524061079Pas encore d'évaluation
- ACE InhibitorDocument19 pagesACE InhibitorApurba Sarker ApuPas encore d'évaluation
- Overview of AnaemiaDocument2 pagesOverview of AnaemiaGerardLumPas encore d'évaluation
- Blood Pressure Regulation-2Document40 pagesBlood Pressure Regulation-2Juliza FelicianoPas encore d'évaluation
- Mental Status: Bates Assessment ToolDocument10 pagesMental Status: Bates Assessment ToolAngela IlustrisimoPas encore d'évaluation
- Adverse Drug EffectsDocument66 pagesAdverse Drug EffectsSuba Ranjana BalaPas encore d'évaluation
- CNS DrugsDocument8 pagesCNS DrugsSheral Aida100% (2)
- Anti-Arrhythmic Agents For Pharmacy PDFDocument41 pagesAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaPas encore d'évaluation
- Adrenergic Receptors ChartDocument1 pageAdrenergic Receptors ChartLeon ChenPas encore d'évaluation
- Anatomy and Physiology of PlacentaDocument5 pagesAnatomy and Physiology of PlacentaAmuPas encore d'évaluation
- Pharmacology of Autonomic Nervous SystemDocument106 pagesPharmacology of Autonomic Nervous Systemoscar3spurgeonPas encore d'évaluation
- DRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesDocument3 pagesDRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesManuel BetancurPas encore d'évaluation
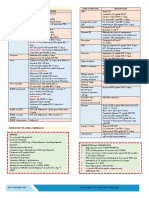
- Respiratory PharmacologyDocument8 pagesRespiratory PharmacologyEPas encore d'évaluation
- 4.l - Respiratory System Pharmacology by IGMRIDocument13 pages4.l - Respiratory System Pharmacology by IGMRIclaw foreSK TeamPas encore d'évaluation
- Defn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andDocument5 pagesDefn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andSambit BeheraPas encore d'évaluation
- Thyroid 2Document58 pagesThyroid 2Seff CausapinPas encore d'évaluation
- Disorders of The Female Reproductive System PDFDocument4 pagesDisorders of The Female Reproductive System PDFSeff CausapinPas encore d'évaluation
- Dem Tickler NotesDocument1 pageDem Tickler NotesSeff CausapinPas encore d'évaluation
- 3 180824051636Document45 pages3 180824051636Seff CausapinPas encore d'évaluation
- Disorders of The Female Reproductive System PDFDocument4 pagesDisorders of The Female Reproductive System PDFSeff CausapinPas encore d'évaluation
- Altitude IllnessDocument4 pagesAltitude IllnessSeff CausapinPas encore d'évaluation
- Hemostasissurgicalbleedingandtransfusion 130707035616 Phpapp02Document42 pagesHemostasissurgicalbleedingandtransfusion 130707035616 Phpapp02Seff CausapinPas encore d'évaluation
- Anterior Pituitary Tumor SyndromesDocument10 pagesAnterior Pituitary Tumor SyndromesSeff CausapinPas encore d'évaluation
- Anterior Pituitary Tumor SyndromesDocument10 pagesAnterior Pituitary Tumor SyndromesSeff CausapinPas encore d'évaluation
- Urinary Tract ObstructionDocument2 pagesUrinary Tract ObstructionSeff CausapinPas encore d'évaluation
- Glomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesDocument6 pagesGlomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesSeff CausapinPas encore d'évaluation
- Lumbar TapDocument4 pagesLumbar TapSeff CausapinPas encore d'évaluation
- Medicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Document3 pagesMedicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Seff CausapinPas encore d'évaluation
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinPas encore d'évaluation
- Abdomen Physical DiagnosisDocument3 pagesAbdomen Physical DiagnosisSeff CausapinPas encore d'évaluation
- Musculoskeletal System Physical DiagnosisDocument4 pagesMusculoskeletal System Physical DiagnosisSeff Causapin100% (1)
- Complete Guide To Physical ExamDocument19 pagesComplete Guide To Physical ExamSeff Causapin100% (2)
- Disorders of The MediastinumDocument1 pageDisorders of The MediastinumSeff CausapinPas encore d'évaluation
- Approach To The PX With CancerDocument7 pagesApproach To The PX With CancerSeff CausapinPas encore d'évaluation
- Peripheral Vascular System Physical DiagnosisDocument3 pagesPeripheral Vascular System Physical DiagnosisSeff Causapin100% (1)
- Clinicopathologic Narrative ReportDocument3 pagesClinicopathologic Narrative ReportSeff CausapinPas encore d'évaluation
- Physical Diagnosis of The ThoraxDocument3 pagesPhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- Physical Diagnosis of Cardiovascular SystemDocument6 pagesPhysical Diagnosis of Cardiovascular SystemSeff Causapin100% (1)
- Pathophysiology of SLEDocument16 pagesPathophysiology of SLESeff CausapinPas encore d'évaluation
- MNGT of AmoebiasisDocument6 pagesMNGT of AmoebiasisSeff CausapinPas encore d'évaluation
- Disturbances in Respiratory FunctionDocument6 pagesDisturbances in Respiratory FunctionSeff CausapinPas encore d'évaluation
- Tubulointerstitial DsesDocument3 pagesTubulointerstitial DsesSeff CausapinPas encore d'évaluation
- Salmon Ellos IsDocument3 pagesSalmon Ellos IsSeff CausapinPas encore d'évaluation
- LeptospirosisDocument2 pagesLeptospirosisSeff CausapinPas encore d'évaluation
- Determining Back Pressure When Sizing For PRV - Relief Devices Forum - Cheresources - Com CommunityDocument5 pagesDetermining Back Pressure When Sizing For PRV - Relief Devices Forum - Cheresources - Com CommunityKyriakos MichalakiPas encore d'évaluation
- 3 NsaidsDocument23 pages3 NsaidsHagai MagaiPas encore d'évaluation
- Kamiastricity - The Effeciency of KamiasDocument15 pagesKamiastricity - The Effeciency of KamiasRobby Lastimosa100% (1)
- E&DPlan 0506Document44 pagesE&DPlan 0506Farhan ShahPas encore d'évaluation
- Structure Test 2Document3 pagesStructure Test 2Seda Aydin100% (1)
- Numericals of ChemistryDocument4 pagesNumericals of ChemistryAakash AkronosPas encore d'évaluation
- Isomerism: Definition-Structural Isomers: Same Molecular Formula Different Structures (Or Structural Formulae)Document13 pagesIsomerism: Definition-Structural Isomers: Same Molecular Formula Different Structures (Or Structural Formulae)Trần Duy Tân100% (1)
- Home Assignment-6 (Practice Problem) Chapter-7Document2 pagesHome Assignment-6 (Practice Problem) Chapter-7Rounak MajumdarPas encore d'évaluation
- Yuanping Wang Chuqin Yu: Preparation and in Vitro Dissolution of Curcumin Tablets,, Zhixiang Gan, Zhongbo XieDocument7 pagesYuanping Wang Chuqin Yu: Preparation and in Vitro Dissolution of Curcumin Tablets,, Zhixiang Gan, Zhongbo XieChristinePas encore d'évaluation
- Thurmalox 8200 Painting SpecificationDocument2 pagesThurmalox 8200 Painting SpecificationFreddy Carl FredricksenPas encore d'évaluation
- PaintDocument28 pagesPaintAnna KateurinaPas encore d'évaluation
- B 921 - 02 - QJKYMQ - ISO 8015 Tolerancing StandardsDocument2 pagesB 921 - 02 - QJKYMQ - ISO 8015 Tolerancing Standardsjameswood20100% (1)
- Chemical Engineering Board Exam PDFDocument3 pagesChemical Engineering Board Exam PDFJohn Leonard FazPas encore d'évaluation
- Mixed-Use Development One Binondo: Moriones St. Cor. Juan Luna St. Binondo, ManilaDocument1 pageMixed-Use Development One Binondo: Moriones St. Cor. Juan Luna St. Binondo, ManilaedwinPas encore d'évaluation
- Addis Ababa University: GeographyDocument6 pagesAddis Ababa University: GeographybereketPas encore d'évaluation
- The Public's Love Affair With Geodes: Rock MineralDocument3 pagesThe Public's Love Affair With Geodes: Rock MineralSerkan KocapinarPas encore d'évaluation
- Reaction PaperDocument2 pagesReaction PaperKimberly Molato0% (1)
- Alakliphiles ProjDocument24 pagesAlakliphiles ProjReshmi Jadwani100% (2)
- Practise School - ChemistryDocument64 pagesPractise School - ChemistrySonakshi BhatiaPas encore d'évaluation
- Primacs TOC Analyser: Chapter 1: IntroductionDocument12 pagesPrimacs TOC Analyser: Chapter 1: IntroductionAnonymous 2LYCWDPuiuPas encore d'évaluation
- Introduction To Antibiotics: Mrs Natasha MahajanDocument17 pagesIntroduction To Antibiotics: Mrs Natasha Mahajannatasha jadhavPas encore d'évaluation
- FDA Checklist: Emergency Ventilation EquipmentDocument2 pagesFDA Checklist: Emergency Ventilation EquipmentRyan DosetarehPas encore d'évaluation
- CM Heavy-Duty Crane Hooks BrochureDocument12 pagesCM Heavy-Duty Crane Hooks Brochuretvmehta01Pas encore d'évaluation
- Chap 03 PPTDocument25 pagesChap 03 PPThk11813Pas encore d'évaluation
- 0620 m23 QP 22-MinDocument14 pages0620 m23 QP 22-Minjelani17fPas encore d'évaluation
- Tappi Extrution Coating and LaminatingDocument26 pagesTappi Extrution Coating and LaminatingKhương HuỳnhPas encore d'évaluation
- Super CatalogDocument189 pagesSuper Catalog윤종주Pas encore d'évaluation