Vous aimerez peut-être aussi
- PIIS1360859220300231Document12 pagesPIIS1360859220300231Максим ВикторовичPas encore d'évaluation
- Management Thoracic Pain 2019Document9 pagesManagement Thoracic Pain 2019Lotte WeggemanPas encore d'évaluation
- Proprioception in Musculoskeletal Rehabilitation2Document10 pagesProprioception in Musculoskeletal Rehabilitation2Santiago Cubillos EscobarPas encore d'évaluation
- Mirror Therapy and Task-Oriented Training For PeopleDocument8 pagesMirror Therapy and Task-Oriented Training For PeopleEmilia LaudaniPas encore d'évaluation
- Bauer 2019Document10 pagesBauer 2019Rafa ZalfaPas encore d'évaluation
- Proprioception in Musculoskeletal Rehabilitation. Part 2: Clinical Assessment and InterventionDocument10 pagesProprioception in Musculoskeletal Rehabilitation. Part 2: Clinical Assessment and InterventionAlejandra VasquezPas encore d'évaluation
- 2010 - Manual Therapy PDFDocument5 pages2010 - Manual Therapy PDFYuzo IgarashiPas encore d'évaluation
- The Effects of Active Break and Postural Shift Interventions On Recovery FromDocument8 pagesThe Effects of Active Break and Postural Shift Interventions On Recovery FromNiko TrogerPas encore d'évaluation
- Validade Diagnostica FRTDocument7 pagesValidade Diagnostica FRTMatheus HackPas encore d'évaluation
- Musculoskeletal Science and PracticeDocument11 pagesMusculoskeletal Science and PracticeAnii warikarPas encore d'évaluation
- The Effect of Cervical Traction Combined With Neural Mobilization On Pain and Disability in Cervical RadiculopathyDocument5 pagesThe Effect of Cervical Traction Combined With Neural Mobilization On Pain and Disability in Cervical RadiculopathyJORGE MANÇOPas encore d'évaluation
- Art - Equilibrio y PropiocepcionDocument7 pagesArt - Equilibrio y PropiocepcionYuLyChPas encore d'évaluation
- Clinical Measurement of Posterior Shoulder ExibilityDocument4 pagesClinical Measurement of Posterior Shoulder ExibilityPrincess Dianna SulitPas encore d'évaluation
- Construct Validity of Lumbar Extension Measures in Mckenzie'S Derangement SyndromeDocument7 pagesConstruct Validity of Lumbar Extension Measures in Mckenzie'S Derangement SyndromeTomáš KrajíčekPas encore d'évaluation
- Balance and Vestibular Rehabilitation: Presented By: Neha Tabbassum Khan M.P.T. 1 Yr (Neuro)Document25 pagesBalance and Vestibular Rehabilitation: Presented By: Neha Tabbassum Khan M.P.T. 1 Yr (Neuro)Vidya VenkitaramanPas encore d'évaluation
- Manual Therapy: Original ArticleDocument6 pagesManual Therapy: Original ArticleRyan SetyantoPas encore d'évaluation
- Wernli K. OSullivan P. Smith A. Campbell A. Kent O. 2020. Movement Posture and Low Back Pain. How Do They RelateDocument19 pagesWernli K. OSullivan P. Smith A. Campbell A. Kent O. 2020. Movement Posture and Low Back Pain. How Do They RelateVizaPas encore d'évaluation
- Constraint-Induced Movement Therapy For People Following Stroke in An Outpatient SettingDocument10 pagesConstraint-Induced Movement Therapy For People Following Stroke in An Outpatient SettingPraneethaPas encore d'évaluation
- 10 1002@pri 1795 PDFDocument6 pages10 1002@pri 1795 PDFJuliano BritoPas encore d'évaluation
- 1 s2.0 S0965229923000833 MainDocument11 pages1 s2.0 S0965229923000833 MaintheophileflorentinPas encore d'évaluation
- A Clinical Test of Lumbopelvic ControlDocument7 pagesA Clinical Test of Lumbopelvic ControlFlávio GuimarãesPas encore d'évaluation
- Manual Therapy: Filip Struyf, Jo Nijs, Stijn Horsten, Sarah Mottram, Steven Truijen, Romain MeeusenDocument6 pagesManual Therapy: Filip Struyf, Jo Nijs, Stijn Horsten, Sarah Mottram, Steven Truijen, Romain MeeusenJorgePas encore d'évaluation
- PTH 662 - Literature Review PaperDocument8 pagesPTH 662 - Literature Review Paperapi-551757456Pas encore d'évaluation
- PNF 22 The Effects of PNF and Trunk Stabilization Robot Training On Trunk Stability and Balance in Patients With Chronic StrokeDocument11 pagesPNF 22 The Effects of PNF and Trunk Stabilization Robot Training On Trunk Stability and Balance in Patients With Chronic StrokeAnonymous j0xAgHs3Pas encore d'évaluation
- Jurnal 1Document9 pagesJurnal 1nur aisahPas encore d'évaluation
- Berg OriginalDocument8 pagesBerg OriginalElizandra Salete Pereira da SilvaPas encore d'évaluation
- LumbarDocument9 pagesLumbarMario Rico GonzálezPas encore d'évaluation
- Cervical StretchingDocument6 pagesCervical StretchingSulthan PhysioPas encore d'évaluation
- Physical Therapy in Sport: Gulcan Harput, Hande Guney-Deniz, John Nyland, Yavuz KocabeyDocument10 pagesPhysical Therapy in Sport: Gulcan Harput, Hande Guney-Deniz, John Nyland, Yavuz KocabeyNaara LibPas encore d'évaluation
- Mechanical Neckpain Article 1Document8 pagesMechanical Neckpain Article 1Zulaikatu MustaphaPas encore d'évaluation
- Omar Maher Shaker 201800746 Trauma AssignmentDocument1 pageOmar Maher Shaker 201800746 Trauma Assignmentomarmaher19Pas encore d'évaluation
- Land 2017 - Effect of Manual Physiotherapy in Homogeneous Individuals With Subacromial Shoulder Impingement - A Randomized Controlled TrialDocument14 pagesLand 2017 - Effect of Manual Physiotherapy in Homogeneous Individuals With Subacromial Shoulder Impingement - A Randomized Controlled TrialJime PEPas encore d'évaluation
- Effect of Motor Control and Strengthening Exercises PDFDocument9 pagesEffect of Motor Control and Strengthening Exercises PDFgonchodiaz1703Pas encore d'évaluation
- 2055 2386 5 14 PDFDocument8 pages2055 2386 5 14 PDFrima rizky nourliaPas encore d'évaluation
- I C M M, M O, H P A M T P - F H P: A R C TDocument9 pagesI C M M, M O, H P A M T P - F H P: A R C TAngie D. AndradesPas encore d'évaluation
- J MSKSP 2017 11 003Document16 pagesJ MSKSP 2017 11 003Rui Pedro PereiraPas encore d'évaluation
- Comparison of Aggressive and Traditional Postoperative Rehabilitation Protocol After Rotator Cuff Repair: A Meta-AnalysisDocument6 pagesComparison of Aggressive and Traditional Postoperative Rehabilitation Protocol After Rotator Cuff Repair: A Meta-AnalysisNico BrantesPas encore d'évaluation
- BBRC Vol 14 No 04 2021-80Document5 pagesBBRC Vol 14 No 04 2021-80Dr Sharique AliPas encore d'évaluation
- Intensive & Critical Care Nursing: Research ArticleDocument7 pagesIntensive & Critical Care Nursing: Research ArticleEviPas encore d'évaluation
- A Test Battery To Measure The Recovery of Voluntary Movement Control Following StrokeDocument4 pagesA Test Battery To Measure The Recovery of Voluntary Movement Control Following StrokeAashish G. ShresthaPas encore d'évaluation
- Moore 2013Document9 pagesMoore 2013Andrés MardonesPas encore d'évaluation
- Effects of Isometric, Eccentric, or Heavy Slow Resistance Exercises On Pain and Function With PTDocument15 pagesEffects of Isometric, Eccentric, or Heavy Slow Resistance Exercises On Pain and Function With PTTomBramboPas encore d'évaluation
- Journal of Bodywork & Movement Therapies: Christopher S. Cayco, Edward James R. Gorgon, Rolando T. LazaroDocument8 pagesJournal of Bodywork & Movement Therapies: Christopher S. Cayco, Edward James R. Gorgon, Rolando T. LazaromaryPas encore d'évaluation
- Effectiveness of StretchingDocument10 pagesEffectiveness of Stretchingاحمد العايديPas encore d'évaluation
- Ankle Inestability Article EvidenceDocument6 pagesAnkle Inestability Article EvidenceAldo Martínez SerranoPas encore d'évaluation
- Cranio-Cervical Exor Muscle Impairment at Maximal, Moderate, and Low Loads Is A Feature of Neck PainDocument6 pagesCranio-Cervical Exor Muscle Impairment at Maximal, Moderate, and Low Loads Is A Feature of Neck PainCristian Alejandro Flores PinuerPas encore d'évaluation
- Expert Therapists Use Specific Clinical Reasoning Processes in The Assessment and Management of Patients With Shoulder Pain: A Qualitative StudyDocument6 pagesExpert Therapists Use Specific Clinical Reasoning Processes in The Assessment and Management of Patients With Shoulder Pain: A Qualitative StudyArdi PrasojoPas encore d'évaluation
- ¿La Frecuencia y La Supervisión Del Entrenamiento Afectan El CumplimientoDocument9 pages¿La Frecuencia y La Supervisión Del Entrenamiento Afectan El CumplimientoFrancisco Javier Luza RamosPas encore d'évaluation
- Which Trunk Inclination Directions Best Predict Multidirectional-Seated Limits of Stability Among Individuals With Spinal Cord Injury?Document8 pagesWhich Trunk Inclination Directions Best Predict Multidirectional-Seated Limits of Stability Among Individuals With Spinal Cord Injury?Chanapass DenduangPas encore d'évaluation
- Acute Effects of Hamstring Stretching On Sagittal Spinal Curvatures and Pelvic TiltDocument10 pagesAcute Effects of Hamstring Stretching On Sagittal Spinal Curvatures and Pelvic TiltOcAn D'scAmpPas encore d'évaluation
- Johnson 2017Document4 pagesJohnson 2017febrian rahmatPas encore d'évaluation
- Tmo en Columna CervicalDocument5 pagesTmo en Columna CervicalIvanMejiaJaramilloPas encore d'évaluation
- Spin LtsDocument12 pagesSpin LtsFederico FragozaPas encore d'évaluation
- The Effects of Bobath-Based Trunk Exercises On Trunk Control, Functional Capacity, Balance, and Gait: A Pilot Randomized Controlled TrialDocument9 pagesThe Effects of Bobath-Based Trunk Exercises On Trunk Control, Functional Capacity, Balance, and Gait: A Pilot Randomized Controlled Trialnandhini raguPas encore d'évaluation
- Diafragma Ant Posterior ChainDocument7 pagesDiafragma Ant Posterior ChainJulijus MotiejunasPas encore d'évaluation
- Test-Re-Test Reliability and Inter-Rater Reliability of A Digital Pelvic Inclinometer in Young, Healthy Males and FemalesDocument15 pagesTest-Re-Test Reliability and Inter-Rater Reliability of A Digital Pelvic Inclinometer in Young, Healthy Males and FemalesfilorpgPas encore d'évaluation
- Artigo - Contenção de TroncoDocument14 pagesArtigo - Contenção de TroncoEduardo LimaPas encore d'évaluation
- MCCSinTEP PublishedPaperDocument7 pagesMCCSinTEP PublishedPaperUCI HUSJPas encore d'évaluation
- Surgical Protocols For Ridge Preservation After Tooth Extraxtion. A Systematic Review.Document17 pagesSurgical Protocols For Ridge Preservation After Tooth Extraxtion. A Systematic Review.Viorel FaneaPas encore d'évaluation
- Sensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCDocument18 pagesSensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCebrahimpanPas encore d'évaluation
- Models For DC MotorsDocument8 pagesModels For DC MotorsebrahimpanPas encore d'évaluation
- Mechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorDocument12 pagesMechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorebrahimpanPas encore d'évaluation
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDocument14 pagesAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanPas encore d'évaluation
- Design and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsDocument12 pagesDesign and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsebrahimpanPas encore d'évaluation
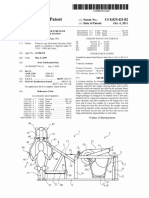
- United States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011Document15 pagesUnited States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011ebrahimpanPas encore d'évaluation
- Spring Over Muscle (SOM) Actuator For Rehabilitation DevicesDocument4 pagesSpring Over Muscle (SOM) Actuator For Rehabilitation DevicesebrahimpanPas encore d'évaluation
- Strain CylindricalDocument4 pagesStrain CylindricalebrahimpanPas encore d'évaluation
- A Review of The Use of Electro-Motor Stimulation in Human MusclesDocument13 pagesA Review of The Use of Electro-Motor Stimulation in Human MusclesebrahimpanPas encore d'évaluation
- Watanabe 2010Document4 pagesWatanabe 2010ebrahimpanPas encore d'évaluation
- I M T: R F V: Sokinetic Uscle Esting Eflections ON Uture EnuesDocument6 pagesI M T: R F V: Sokinetic Uscle Esting Eflections ON Uture EnuesebrahimpanPas encore d'évaluation
- An Assisted Waist Supporter For Vertebral RehabilitationDocument2 pagesAn Assisted Waist Supporter For Vertebral RehabilitationebrahimpanPas encore d'évaluation
- Jomms 08Document20 pagesJomms 08ebrahimpanPas encore d'évaluation
- 06 Linear Elasticity 03 Anisotropy PDFDocument11 pages06 Linear Elasticity 03 Anisotropy PDFebrahimpanPas encore d'évaluation
- Zenoah g320rc Owners Manual DDMDocument28 pagesZenoah g320rc Owners Manual DDMSunthron SomchaiPas encore d'évaluation
- Tip Convolution Lang98Document5 pagesTip Convolution Lang98ebrahimpanPas encore d'évaluation
- Upper Respiratory Tract InfectionDocument3 pagesUpper Respiratory Tract Infectionmcvirgo014100% (1)
- Post Dam and Relief Chamber FullDocument35 pagesPost Dam and Relief Chamber FullnaomiPas encore d'évaluation
- User Manual For Applications Xformer Exe EnglishLightDocument51 pagesUser Manual For Applications Xformer Exe EnglishLightNunoClaudinoPas encore d'évaluation
- Chapter 16 - Nur-WPS OfficeDocument11 pagesChapter 16 - Nur-WPS Officemichelle marquezPas encore d'évaluation
- Pharmaceutical SciencesDocument5 pagesPharmaceutical SciencesiajpsPas encore d'évaluation
- Laporan Divisi Nefrologi 3 Maret 2020Document18 pagesLaporan Divisi Nefrologi 3 Maret 2020annisanangPas encore d'évaluation
- Home Boddies TACTILEDocument52 pagesHome Boddies TACTILECosmin PavelPas encore d'évaluation
- Amoebiasis NCPDocument3 pagesAmoebiasis NCPRellie CastroPas encore d'évaluation
- Stroke (Cerebrovascular Accident) : 1. QXCI Treatment PossibilitiesDocument5 pagesStroke (Cerebrovascular Accident) : 1. QXCI Treatment PossibilitiesEnrique Gonzalez Marquier100% (1)
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFDocument94 pages861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosPas encore d'évaluation
- Introductory Lecture Series: The Anesthesia MachineDocument37 pagesIntroductory Lecture Series: The Anesthesia MachineDenny RamdhanPas encore d'évaluation
- 2021 Nexus Pharma Injection Price List FinalDocument5 pages2021 Nexus Pharma Injection Price List FinalRyu SanurPas encore d'évaluation
- Initial Nurse Patient InteractionDocument1 pageInitial Nurse Patient InteractionBryan Jay Carlo PañaPas encore d'évaluation
- Optimum Detox Foot Pads, Natural Cleansing Ginger Detox Foot PatchesDocument1 pageOptimum Detox Foot Pads, Natural Cleansing Ginger Detox Foot PatchesBrooke GuntherPas encore d'évaluation
- Klinefelters SyndromeDocument2 pagesKlinefelters SyndromeAlexandra Gabriella ZawisnyPas encore d'évaluation
- Management of Infective EndocarditisDocument14 pagesManagement of Infective Endocarditismhafzam2020Pas encore d'évaluation
- List of Herbal Ingredients Which Are Prohibited or Restricted in MedicinesDocument12 pagesList of Herbal Ingredients Which Are Prohibited or Restricted in MedicinesEtra PublishingPas encore d'évaluation
- Documentary Requirements and Format of Simplified CSHPDocument1 pageDocumentary Requirements and Format of Simplified CSHPRhalf AbnePas encore d'évaluation
- At The PharmacyDocument6 pagesAt The PharmacyCristian González GonzálezPas encore d'évaluation
- Neuroscience: Science of The Brain in PolishDocument72 pagesNeuroscience: Science of The Brain in PolishInternational Brain Research Organization100% (1)
- Case Study - DR EldaDocument3 pagesCase Study - DR EldaShashi KumarPas encore d'évaluation
- Buffer Systems in The Body: Protein Buffers in Blood Plasma and CellsDocument11 pagesBuffer Systems in The Body: Protein Buffers in Blood Plasma and CellsK Jayakumar KandasamyPas encore d'évaluation
- Republic Act MnemonicsDocument3 pagesRepublic Act MnemonicsJill P100% (1)
- Neurology Case SheetDocument9 pagesNeurology Case SheetAshwaq TpPas encore d'évaluation
- Comprehensive Revision Test - Basics 1Document16 pagesComprehensive Revision Test - Basics 1drpnnreddyPas encore d'évaluation
- The Effects of Skin Bleach in SocietyDocument8 pagesThe Effects of Skin Bleach in SocietySalma BahPas encore d'évaluation
- BC CancerDocument42 pagesBC CancerIsal SparrowPas encore d'évaluation
- Cutaneous Candidiasis - An Evidence-Based Review of Topical and Systemic Treatments To Inform Clinical PracticeDocument11 pagesCutaneous Candidiasis - An Evidence-Based Review of Topical and Systemic Treatments To Inform Clinical PracticeRose ParkPas encore d'évaluation
- Porco EspinhoDocument9 pagesPorco EspinhoLeticia LimaPas encore d'évaluation
- UCSI 2017 Building DirectoryDocument11 pagesUCSI 2017 Building DirectorySeanPas encore d'évaluation