Vous aimerez peut-être aussi
- Transcript Emily Fletcher Greater Sex Better Sleep With Ziva Meditation 224 PDFDocument40 pagesTranscript Emily Fletcher Greater Sex Better Sleep With Ziva Meditation 224 PDFLacramioara Ionescu100% (1)
- Partnership in Health and Social Care Analysis Social Work EssayDocument9 pagesPartnership in Health and Social Care Analysis Social Work EssayHND Assignment HelpPas encore d'évaluation
- Strategies to Explore Ways to Improve Efficiency While Reducing Health Care CostsD'EverandStrategies to Explore Ways to Improve Efficiency While Reducing Health Care CostsPas encore d'évaluation
- Offshore Risk Management - Security Assessment For Offshore Oil PDFDocument26 pagesOffshore Risk Management - Security Assessment For Offshore Oil PDFlightangeldavidPas encore d'évaluation
- Globalisation and ManagementDocument6 pagesGlobalisation and ManagementmickyPas encore d'évaluation
- Change InitiativeDocument7 pagesChange InitiativeWajiha ShaikhPas encore d'évaluation
- Unit 3 Health and Social CareDocument22 pagesUnit 3 Health and Social Carearies usamaPas encore d'évaluation
- Time To Learn. Understanding Patient Centered CareDocument7 pagesTime To Learn. Understanding Patient Centered CareIstianah EsPas encore d'évaluation
- An Introduction To Evidence-Based NursinDocument8 pagesAn Introduction To Evidence-Based NursinAli MaqsudiPas encore d'évaluation
- Enhancing Communication M LITA 18052979Document7 pagesEnhancing Communication M LITA 18052979Mel MercerPas encore d'évaluation
- Student Shadowing ReportDocument3 pagesStudent Shadowing Reportapi-438107530Pas encore d'évaluation
- Leadership in NHS BMJ 2019Document4 pagesLeadership in NHS BMJ 2019Supriya KapasPas encore d'évaluation
- Multidisciplinary Team and Pharmacists Role in That TeamDocument5 pagesMultidisciplinary Team and Pharmacists Role in That TeamTimothy OgomaPas encore d'évaluation
- Long Term Conditions Collaborative: Improving Self Management SupportDocument34 pagesLong Term Conditions Collaborative: Improving Self Management SupportDefi DestyawenyPas encore d'évaluation
- Team Delivery Report PDFDocument32 pagesTeam Delivery Report PDFwendyPas encore d'évaluation
- Climate Change, What Is It - Understanding The Basic Facts About Global WarmingDocument23 pagesClimate Change, What Is It - Understanding The Basic Facts About Global WarmingFer OssPas encore d'évaluation
- Formulation: Vision and Mission: Session 2 Ratna Roostika, PHDDocument25 pagesFormulation: Vision and Mission: Session 2 Ratna Roostika, PHDAnonymous iiWoac8kPas encore d'évaluation
- Health Care Workers Motivation and Retention Approaches of Health Workersin Ethiopia A Scoping ReviewDocument7 pagesHealth Care Workers Motivation and Retention Approaches of Health Workersin Ethiopia A Scoping ReviewBSIT2C-REYES, ChristianPas encore d'évaluation
- Working in Partnership in Health and Social CareDocument10 pagesWorking in Partnership in Health and Social Carehossain alviPas encore d'évaluation
- EBMDocument636 pagesEBMDaniel SalaPas encore d'évaluation
- Microbiology-Disinfectants Lab ReportDocument2 pagesMicrobiology-Disinfectants Lab Reportsaraebo25% (4)
- The Transformation of Academic Health Centers: Meeting the Challenges of Healthcare’s Changing LandscapeD'EverandThe Transformation of Academic Health Centers: Meeting the Challenges of Healthcare’s Changing LandscapePas encore d'évaluation
- Drug Awareness and Prevention Program PDFDocument6 pagesDrug Awareness and Prevention Program PDFMarcos Bulay OgPas encore d'évaluation
- Applying Lewins Change Management Theory To The Implementation of Bar-Coded Medication AdministrationDocument6 pagesApplying Lewins Change Management Theory To The Implementation of Bar-Coded Medication AdministrationgergisPas encore d'évaluation
- Professional Accountability in NursingDocument4 pagesProfessional Accountability in NursingJohn N MwangiPas encore d'évaluation
- Conference Program: 4th Asia Pacific Regional Conference On Health Impact Assessment (HIA), Seoul, South Korea, 9-11 October 2012Document56 pagesConference Program: 4th Asia Pacific Regional Conference On Health Impact Assessment (HIA), Seoul, South Korea, 9-11 October 2012ADB Health Sector GroupPas encore d'évaluation
- C CDocument2 pagesC Capi-354302626Pas encore d'évaluation
- Competencies and CapabilitiesDocument10 pagesCompetencies and CapabilitiesMarwan BecharaPas encore d'évaluation
- Final EssayDocument9 pagesFinal Essayapi-383024083Pas encore d'évaluation
- Doctor Patient RelationshipDocument4 pagesDoctor Patient RelationshipvishnuPas encore d'évaluation
- The Dangers of ComplacencyDocument3 pagesThe Dangers of Complacencyegahmulia100% (2)
- Genigraphics Poster Template 36x36Document1 pageGenigraphics Poster Template 36x36Iqbal Hossain NoyonPas encore d'évaluation
- NS 622 AssignmentDocument16 pagesNS 622 AssignmentGareth McKnightPas encore d'évaluation
- Organizational Structure and Culture PaperDocument2 pagesOrganizational Structure and Culture PaperFrancesca Simiriglio- BeebePas encore d'évaluation
- Analysis of Organisational Culture and Management of SamsungDocument4 pagesAnalysis of Organisational Culture and Management of SamsungEun AhPas encore d'évaluation
- Ahrq 2004 PDFDocument74 pagesAhrq 2004 PDFDelly TunggalPas encore d'évaluation
- EOQ - P.AgroDocument72 pagesEOQ - P.AgrokartikPas encore d'évaluation
- Molly's Case StudyDocument10 pagesMolly's Case StudyYounas BhattiPas encore d'évaluation
- WFCCN 2.0 Chapter 10 Family Centred Care 2nd Edition EbookDocument43 pagesWFCCN 2.0 Chapter 10 Family Centred Care 2nd Edition Ebookproners samratulangiPas encore d'évaluation
- WBS Graphical TemplateDocument1 pageWBS Graphical TemplateJaveed A. KhanPas encore d'évaluation
- European Strategic Directions Strengthening Nursing Midwifery Health2020 en REV1Document35 pagesEuropean Strategic Directions Strengthening Nursing Midwifery Health2020 en REV1Catalina StoicescuPas encore d'évaluation
- National Health PolicyDocument22 pagesNational Health PolicyAncy Varkey100% (2)
- SVH Strategic Plan 2012 PDFDocument42 pagesSVH Strategic Plan 2012 PDFRichard HutasoitPas encore d'évaluation
- NHS (HEE) - Mental Wellbeing Commission ReportDocument98 pagesNHS (HEE) - Mental Wellbeing Commission ReportMax EvansPas encore d'évaluation
- Quality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDocument37 pagesQuality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDewi ListyoriniPas encore d'évaluation
- Why Do You Think Nursing Is A Global ProfessionDocument2 pagesWhy Do You Think Nursing Is A Global ProfessionMae Usquisa100% (1)
- Leadership PortfolioDocument7 pagesLeadership PortfolioKaylea AlgirePas encore d'évaluation
- Sample Report On Facilitating Change in Health and Social Care by Instant Essay WritingDocument17 pagesSample Report On Facilitating Change in Health and Social Care by Instant Essay WritingInstant Essay WritingPas encore d'évaluation
- Order-Winning and Order-Qualifying CriteriaDocument3 pagesOrder-Winning and Order-Qualifying CriteriaJesica MaryPas encore d'évaluation
- Hidden CurriculumDocument20 pagesHidden CurriculumTodd Patrick MarekPas encore d'évaluation
- Assingnment 3 775Document17 pagesAssingnment 3 775madhwa79Pas encore d'évaluation
- Geneticsgenomics in Nursing and Health CareDocument15 pagesGeneticsgenomics in Nursing and Health Careapi-215814528Pas encore d'évaluation
- Government Regulatory Agencies - HHSDocument15 pagesGovernment Regulatory Agencies - HHSJocelyn GarciaPas encore d'évaluation
- Master in Hospital MGT - SyllabusDocument65 pagesMaster in Hospital MGT - SyllabusArpit Gupta100% (1)
- Stability and Change in Managerial Work Values - Ralston Et Al - 2006Document47 pagesStability and Change in Managerial Work Values - Ralston Et Al - 2006alanwilPas encore d'évaluation
- Planning in Healthcare OrganizationsDocument3 pagesPlanning in Healthcare Organizationssarah ahmedPas encore d'évaluation
- Describe Four You Would Implement When Managing A Team To Ensure That All Members Are Clear On Their Responsibilities and RequirementsDocument12 pagesDescribe Four You Would Implement When Managing A Team To Ensure That All Members Are Clear On Their Responsibilities and RequirementssumanpremPas encore d'évaluation
- Nurs FPX 4050 Assessment 1 Preliminary Care Coordination PlanDocument4 pagesNurs FPX 4050 Assessment 1 Preliminary Care Coordination PlanEmma Watson100% (1)
- Microsoft Balanced Scorecard Framework5Document33 pagesMicrosoft Balanced Scorecard Framework5abcdePas encore d'évaluation
- Plis.L.final CapstoneDocument44 pagesPlis.L.final CapstoneDianEsvaniPas encore d'évaluation
- Unit 29 Health PromotionDocument4 pagesUnit 29 Health Promotionchandni0810100% (1)
- Ealth Ystem Eforms: 9.1 Summary of Recent and Planned ReformsDocument6 pagesEalth Ystem Eforms: 9.1 Summary of Recent and Planned ReformsMohamed SalahPas encore d'évaluation
- Realizing The Potential of Nurses Role in Genetics and Genomic Health Care - An Integrated Review of The LiteratureDocument5 pagesRealizing The Potential of Nurses Role in Genetics and Genomic Health Care - An Integrated Review of The LiteratureIOSRjournalPas encore d'évaluation
- Worksheet Normal Distribution PDFDocument3 pagesWorksheet Normal Distribution PDFJustin Eduard MarzanPas encore d'évaluation
- Clasp BDJDocument11 pagesClasp BDJAtiq RehmanPas encore d'évaluation
- Factors Affecting Demand For Soft DrinksDocument8 pagesFactors Affecting Demand For Soft Drinksخلود البطاحPas encore d'évaluation
- Town Planning: Q. Identify The Problems in India Regarding Town PlanningDocument8 pagesTown Planning: Q. Identify The Problems in India Regarding Town PlanningYogesh BhardwajPas encore d'évaluation
- Assessment Environmental Toxicity ReportDocument43 pagesAssessment Environmental Toxicity ReportStan LeePas encore d'évaluation
- PI e UREA 15Document2 pagesPI e UREA 15dewi asnaniPas encore d'évaluation
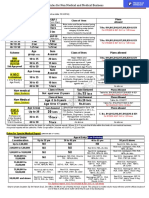
- Rules For Non Medical BusinessDocument1 pageRules For Non Medical BusinessAbhijit AminpurPas encore d'évaluation
- Restobar FSDocument58 pagesRestobar FSGabrielle Alonzo100% (1)
- Dwnload Full Wardlaws Contemporary Nutrition A Functional Approach 5th Edition Wardlaw Test Bank PDFDocument36 pagesDwnload Full Wardlaws Contemporary Nutrition A Functional Approach 5th Edition Wardlaw Test Bank PDFamoeboid.amvis.uiem100% (9)
- Sce550 PresentDocument57 pagesSce550 Presentapi-289477817Pas encore d'évaluation
- Referat Limba Engleză-Zidaroiu Ionuț-EduardDocument6 pagesReferat Limba Engleză-Zidaroiu Ionuț-EduardEduard IonutPas encore d'évaluation
- P.E & Health G11-Q1-M7Document13 pagesP.E & Health G11-Q1-M7John Gerald CantancioPas encore d'évaluation
- Chap 4Document14 pagesChap 4Bambi AlaizaPas encore d'évaluation
- PI - Standard - Seafood Processing - Issue 5.0 - 1-February-2019Document65 pagesPI - Standard - Seafood Processing - Issue 5.0 - 1-February-2019pebru yuwono0% (1)
- Fundamentals of Nursing - Nurse As ProfessionDocument7 pagesFundamentals of Nursing - Nurse As ProfessionDarryl C. LocañasPas encore d'évaluation
- Paper7 Syl22 Dec23 Set2 SolDocument20 pagesPaper7 Syl22 Dec23 Set2 SolAkash AgarwalPas encore d'évaluation
- Spoon University Nutrition GuideDocument80 pagesSpoon University Nutrition GuidermdelmandoPas encore d'évaluation
- Stress and Coping Styles To StudentsDocument8 pagesStress and Coping Styles To StudentsArien Kaye VallarPas encore d'évaluation
- Post-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceDocument17 pagesPost-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceMari PaoPas encore d'évaluation
- Id ProofDocument3 pagesId ProofSagar MittaPas encore d'évaluation
- Health & Illness FinalDocument16 pagesHealth & Illness FinalAJPas encore d'évaluation
- Texas Medicaid and CHIP Provider FAQsDocument4 pagesTexas Medicaid and CHIP Provider FAQsangelina smithPas encore d'évaluation
- THE Center: Anxiety DisordersDocument13 pagesTHE Center: Anxiety DisordersOti VuraPas encore d'évaluation
- Turner 1st SEM at FinalDocument102 pagesTurner 1st SEM at FinalSashikant Sharma100% (1)
- BISWAS Vol 3, Issue 2Document225 pagesBISWAS Vol 3, Issue 2Vinayak guptaPas encore d'évaluation
- Ob MidtermDocument5 pagesOb MidtermSheila Tolentino-BelanioPas encore d'évaluation