Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Working Paper: Child Malnutrition and Antenatal Care Evidence From Three Latin American CountriesDocument28 pagesWorking Paper: Child Malnutrition and Antenatal Care Evidence From Three Latin American CountriesKomala SariPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Consultation On: Improving Measurement of The Quality of Maternal, Newborn and Child Care in Health FacilitiesDocument43 pagesConsultation On: Improving Measurement of The Quality of Maternal, Newborn and Child Care in Health FacilitiesKomala SariPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Determinants of The Number of Antenatal Visits in A Metropolitan RegionDocument9 pagesDeterminants of The Number of Antenatal Visits in A Metropolitan RegionKomala SariPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Aguayo Et Al-2016-Maternal & Child NutritionDocument20 pagesAguayo Et Al-2016-Maternal & Child NutritionKomala SariPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Antenatal and Early Infant Predictors of Postnatal Growth in Rural Vietnam: A Prospective Cohort StudyDocument10 pagesAntenatal and Early Infant Predictors of Postnatal Growth in Rural Vietnam: A Prospective Cohort StudyKomala SariPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Prevalence and Factors Associated With Stunting and Excess Weight in Children Aged 0-5 Years From The Brazilian Semi-Arid RegionDocument8 pagesPrevalence and Factors Associated With Stunting and Excess Weight in Children Aged 0-5 Years From The Brazilian Semi-Arid RegionKomala SariPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- 1 s2.0 S0899900714005498 MainDocument6 pages1 s2.0 S0899900714005498 MainKomala SariPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- International Journal of Depression and Anxiety SRDocument8 pagesInternational Journal of Depression and Anxiety SRKomala SariPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- HOMO - Journal of Comparative Human BiologyDocument6 pagesHOMO - Journal of Comparative Human BiologyKomala SariPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- AssociationofmaternalnutritionknowledgeandchildDocument7 pagesAssociationofmaternalnutritionknowledgeandchildKomala SariPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Hospital Majapahit Vol 5 No. 1 Pebruari 2013Document15 pagesHospital Majapahit Vol 5 No. 1 Pebruari 2013Komala SariPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Emotional Health and Pregnancy: A First Steps Guide ToDocument27 pagesEmotional Health and Pregnancy: A First Steps Guide ToKomala SariPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Pre-Partum Exercise Program Using Motion-Based Games: Project TitleDocument5 pagesPre-Partum Exercise Program Using Motion-Based Games: Project TitleKomala SariPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Britishjournalofpsychiatry BRITISHJOURNALOFPSYCHIATRY (2002), 180,502 508 (2 0 0 2), 1 8 0, 5 0 2 5 0 8Document8 pagesBritishjournalofpsychiatry BRITISHJOURNALOFPSYCHIATRY (2002), 180,502 508 (2 0 0 2), 1 8 0, 5 0 2 5 0 8Komala SariPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- 14 BookcabeDocument26 pages14 BookcabeGregorius Manoga BanjarnahorPas encore d'évaluation
- Clinical Implications of Tumor Necrosis Factor-Alpha, Interleukin-6 and Resistin in Coronary Artery DiseaseDocument7 pagesClinical Implications of Tumor Necrosis Factor-Alpha, Interleukin-6 and Resistin in Coronary Artery DiseaseKomala SariPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Women's Health Booklet 1-10Document16 pagesWomen's Health Booklet 1-10Komala SariPas encore d'évaluation
- Fetal Distress 10: Suresh TharmaratnamDocument18 pagesFetal Distress 10: Suresh Tharmaratnamyenni anggrainiPas encore d'évaluation
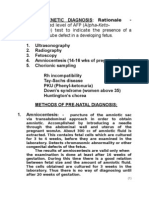
- Prenatal DiagnosisDocument5 pagesPrenatal Diagnosissarguss14Pas encore d'évaluation
- 1.neonatal Feeding Record For Breastfeeding Establishtment - Lily RundjanDocument25 pages1.neonatal Feeding Record For Breastfeeding Establishtment - Lily RundjanRhyno FebriyantoPas encore d'évaluation
- NHSRC - Operational Guidelines On Maternal and Newborn HealthDocument46 pagesNHSRC - Operational Guidelines On Maternal and Newborn HealthNational Child Health Resource Centre (NCHRC)Pas encore d'évaluation
- Fibroid With PregnancyDocument5 pagesFibroid With PregnancyvaishaliPas encore d'évaluation
- Daftar Pustaka MiomaDocument2 pagesDaftar Pustaka Mioma2tialawiPas encore d'évaluation
- Komplikasi Kala III PersalinanDocument27 pagesKomplikasi Kala III Persalinanfebryana wulandariPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- CV Europass CaprosDocument3 pagesCV Europass CaprosCristinaCaprosPas encore d'évaluation
- Assessment of Fetal G&DDocument75 pagesAssessment of Fetal G&DHillary Praise AquinoPas encore d'évaluation
- Vaginal Birth After Two Caesarean Sections (VBAC-2) - A Systematic Review With Meta-Analysis of Success Rate and Adverse Outcomes of VBAC-2 Versus VB..Document2 pagesVaginal Birth After Two Caesarean Sections (VBAC-2) - A Systematic Review With Meta-Analysis of Success Rate and Adverse Outcomes of VBAC-2 Versus VB..mila.diaPas encore d'évaluation
- Narinig Kaya Nila Ang: Tsismis??Document27 pagesNarinig Kaya Nila Ang: Tsismis??iammerbinpransiskoPas encore d'évaluation
- Human Artificial InseminationDocument13 pagesHuman Artificial InseminationMary Joy JunioPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Preterm Charts Combined BoysDocument1 pagePreterm Charts Combined BoysEnny AndrianiPas encore d'évaluation
- Garbhini PareekshaDocument6 pagesGarbhini Pareekshaashutoshjha529Pas encore d'évaluation
- First Versus Second Trimester Mean Platelet Volume and Uric Acid For Prediction of Preeclampsia in Women at Moderate and Low RiskDocument8 pagesFirst Versus Second Trimester Mean Platelet Volume and Uric Acid For Prediction of Preeclampsia in Women at Moderate and Low RiskWael GaberPas encore d'évaluation
- Prom 1Document48 pagesProm 1Tesfahun TeklePas encore d'évaluation
- Delivery Room DutyDocument5 pagesDelivery Room DutyConi Gerenia GamayaoPas encore d'évaluation
- Acupuncture and Acupressure in LaborDocument5 pagesAcupuncture and Acupressure in LaborAstri YuliandiniPas encore d'évaluation
- Breech PresentationDocument29 pagesBreech PresentationSrikitta DanieliaPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Women Harassment & Child LabourDocument36 pagesWomen Harassment & Child LabourAbilash IyerPas encore d'évaluation
- Isuog Guideline IugrDocument15 pagesIsuog Guideline IugrericPas encore d'évaluation
- Record of Actual Delivery HandledDocument2 pagesRecord of Actual Delivery HandledPatricia Ann Salazar RnPas encore d'évaluation
- DED SPPAMC Briefer 1Document71 pagesDED SPPAMC Briefer 1Arlyn AyagPas encore d'évaluation
- Maternal Health and Its Influences On Child HealthDocument83 pagesMaternal Health and Its Influences On Child HealthSangpuii HmarPas encore d'évaluation
- IUFDDocument2 pagesIUFDnurseon0% (1)
- Prenatal CareDocument16 pagesPrenatal CareMark MaPas encore d'évaluation
- Professional Regulation Commission: Board of MidwiferyDocument4 pagesProfessional Regulation Commission: Board of MidwiferyMohammadAbdullahLawanzaPas encore d'évaluation
- Health: Quarter 4 - Module 4b: Professional Health Career Planning Health PathwaysDocument14 pagesHealth: Quarter 4 - Module 4b: Professional Health Career Planning Health PathwaysMarlon CabugasonPas encore d'évaluation
- Prolong LabourDocument5 pagesProlong LabourNishaThakuri100% (1)
- Amniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingDocument19 pagesAmniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingPoonam RanaPas encore d'évaluation
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductD'EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductÉvaluation : 5 sur 5 étoiles5/5 (31)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeD'EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromePas encore d'évaluation
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionD'EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)