Vous aimerez peut-être aussi
- Micro - para FINALDocument53 pagesMicro - para FINALfilchibuff94% (18)
- General Awareness of Pathology With Special Reference To Typhoid DiseaseDocument41 pagesGeneral Awareness of Pathology With Special Reference To Typhoid DiseaseNiveditaPandeyPas encore d'évaluation
- Dengue FeverDocument9 pagesDengue FeverRichardDumlaoPas encore d'évaluation
- Gilut Herpes ZosteRDocument24 pagesGilut Herpes ZosteRdimasahadiantoPas encore d'évaluation
- MaleriaDocument41 pagesMaleriadeepak_143Pas encore d'évaluation
- Approach To Renal BiopsyDocument77 pagesApproach To Renal BiopsySandeep Kumar VushikamallaPas encore d'évaluation
- Antigen Antibody ReactionDocument16 pagesAntigen Antibody ReactionNadzierah RazakPas encore d'évaluation
- Signs and Symptoms: Dengue Fever, Also Known As Breakbone Fever, Is ADocument8 pagesSigns and Symptoms: Dengue Fever, Also Known As Breakbone Fever, Is ALutfi AuliaPas encore d'évaluation
- Bacterial MeningitisDocument1 pageBacterial MeningitisDavid HylandPas encore d'évaluation
- HIV AwarenessDocument35 pagesHIV AwarenessCadine DavisPas encore d'évaluation
- Lecture 1 - InfluenzaDocument67 pagesLecture 1 - InfluenzaShaimaa AbdulkadirPas encore d'évaluation
- By Hemant Sharma Tuberculosis: Latent TB. in This Condition, You Have A TB Infection, But The Bacteria RemainDocument8 pagesBy Hemant Sharma Tuberculosis: Latent TB. in This Condition, You Have A TB Infection, But The Bacteria RemainHemant SharmaPas encore d'évaluation
- Physical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsDocument12 pagesPhysical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsNaomi AnastacioPas encore d'évaluation
- Pharmacovigilance Programme of India The Journey Travelled and The Way ForwardDocument8 pagesPharmacovigilance Programme of India The Journey Travelled and The Way ForwardPreeti KharbPas encore d'évaluation
- TyphoidDocument13 pagesTyphoidMayuri VohraPas encore d'évaluation
- Dengue Fever: DR - J Un S Ay, DR - TupasDocument61 pagesDengue Fever: DR - J Un S Ay, DR - TupasRenette UyPas encore d'évaluation
- Gas Gangrene.Document24 pagesGas Gangrene.Jared GreenPas encore d'évaluation
- Food ProductionDocument9 pagesFood ProductionBharat dhusiyaPas encore d'évaluation
- Genetic DisorderDocument13 pagesGenetic DisorderLucreatia RynjahPas encore d'évaluation
- Typhoid FeverDocument5 pagesTyphoid FeverNaziha InaamPas encore d'évaluation
- Neisseria GonorrhoeaeDocument28 pagesNeisseria GonorrhoeaeRoni Ananda Perwira HarahapPas encore d'évaluation
- EncephalitisDocument27 pagesEncephalitisHasRoni Fathurrahman100% (1)
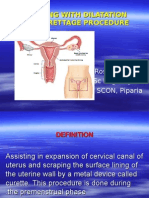
- Assisting With Dilatation and Curettage ProcedureDocument18 pagesAssisting With Dilatation and Curettage ProcedureRoselineTiggaPas encore d'évaluation
- Nanotechnology PDFDocument6 pagesNanotechnology PDFJaneaPas encore d'évaluation
- Nosocomial Infection?Document4 pagesNosocomial Infection?Sara APas encore d'évaluation
- Knowledge, Attitude and Practice About Covid-19 and Vaccine Acceptance Among Family Physician in Al-MadinahDocument9 pagesKnowledge, Attitude and Practice About Covid-19 and Vaccine Acceptance Among Family Physician in Al-MadinahIJAR JOURNALPas encore d'évaluation
- A Brief Note On: Chicken PoxDocument29 pagesA Brief Note On: Chicken PoxRemesh ChandranPas encore d'évaluation
- IGNOU MSCCFT Block-1Document180 pagesIGNOU MSCCFT Block-1Dr. Megha RichhariyaPas encore d'évaluation
- Case 10 Hiv-AidsDocument47 pagesCase 10 Hiv-AidsErikah Eirah BeloriaPas encore d'évaluation
- Design & Simulation of Moving Message Display Using MicrocontrollerDocument67 pagesDesign & Simulation of Moving Message Display Using MicrocontrollerAbhi LekhrajaniPas encore d'évaluation
- ElephantiasisDocument23 pagesElephantiasisNitin0% (1)
- Grand Case DengueDocument14 pagesGrand Case DengueShell BalanguePas encore d'évaluation
- Food PoisoningDocument19 pagesFood PoisoningHemanathan PraemPas encore d'évaluation
- Lesson Plan On Preterm CareDocument4 pagesLesson Plan On Preterm CarePabhat KumarPas encore d'évaluation
- Mrs - PradnyaJadhav (SSKJCN)Document15 pagesMrs - PradnyaJadhav (SSKJCN)pia espanillo100% (1)
- Article On DengueDocument6 pagesArticle On Dengueاحمد احمدPas encore d'évaluation
- Market Share of Dabur Real JuiceDocument66 pagesMarket Share of Dabur Real Juicesushmit raj badolaPas encore d'évaluation
- Integral Building Services PDFDocument5 pagesIntegral Building Services PDFKrish DoodnauthPas encore d'évaluation
- Zika Virus Thesis CHAP-1-2-3 8-26-16Document43 pagesZika Virus Thesis CHAP-1-2-3 8-26-16Richard RL100% (3)
- Shreya Keshari PDFDocument75 pagesShreya Keshari PDFANKIT SINGHPas encore d'évaluation
- Nephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearDocument28 pagesNephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearMaria YaseenPas encore d'évaluation
- MalariaDocument4 pagesMalariaAna May Ramas DelgadoPas encore d'évaluation
- CHICKENPOXDocument32 pagesCHICKENPOXCharlz ZipaganPas encore d'évaluation
- GANGRENE3Document16 pagesGANGRENE3faizi gPas encore d'évaluation
- BANS-184 Important QuestionsDocument31 pagesBANS-184 Important QuestionsRahul Singh RajputPas encore d'évaluation
- DemonetizationDocument27 pagesDemonetizationSuman PoudelPas encore d'évaluation
- Scrub Typhus Guideline On Prevention and ControlDocument3 pagesScrub Typhus Guideline On Prevention and ControlVir balPas encore d'évaluation
- Universal Immunization ProgrammeDocument8 pagesUniversal Immunization ProgrammeNagaraj ReddyPas encore d'évaluation
- Typhoid FeverDocument8 pagesTyphoid FeverKomang Mery100% (1)
- 13.format - App-Hand Anthropometry and Grip StrengthDocument6 pages13.format - App-Hand Anthropometry and Grip StrengthImpact JournalsPas encore d'évaluation
- Olympic Games & FULLDocument8 pagesOlympic Games & FULLAnjum Ansh KhanPas encore d'évaluation
- Family Law AssignmentDocument2 pagesFamily Law Assignmentisha04tyagiPas encore d'évaluation
- Mental Health Services in IndiaDocument10 pagesMental Health Services in IndiaMr cholaPas encore d'évaluation
- Project Seminar Hospice FedoraDocument3 pagesProject Seminar Hospice FedoralalithaPas encore d'évaluation
- 7 Developmental, Genetic, & Pediatric DiseaseDocument62 pages7 Developmental, Genetic, & Pediatric DiseasecamsfPas encore d'évaluation
- Drug Resistant TuberculosisDocument58 pagesDrug Resistant TuberculosisbharatnarayananPas encore d'évaluation
- Emerging and Reemerging Infectious DiseasesDocument25 pagesEmerging and Reemerging Infectious DiseasesNorberto Francisco BaldiPas encore d'évaluation
- Dengue MedscapeDocument58 pagesDengue MedscapearuhulaminiPas encore d'évaluation
- Dengue MedscapeDocument36 pagesDengue Medscapejeanne_mbPas encore d'évaluation
- Dengue MedscapeDocument3 pagesDengue MedscapekathleenvkPas encore d'évaluation
- Synergistic Effect of Lantana CamaraDocument5 pagesSynergistic Effect of Lantana CamaraMarlon Sta. CatalinaPas encore d'évaluation
- Dengue RDT Laboratory Request FormDocument1 pageDengue RDT Laboratory Request FormJosanne Wadwadan De CastroPas encore d'évaluation
- 205 CS - Dengue FeverDocument39 pages205 CS - Dengue FeverMarielle Mae TanPas encore d'évaluation
- Research PaperDocument5 pagesResearch PaperLyn Niño100% (1)
- Fever in Children 2010Document27 pagesFever in Children 2010adystiPas encore d'évaluation
- Epidemiologi Skrining DBD Puskesmas Banjarbaru Utara (English)Document11 pagesEpidemiologi Skrining DBD Puskesmas Banjarbaru Utara (English)rinaaanggraini_Pas encore d'évaluation
- Dengue FeverDocument1 pageDengue Feverapi-266482250Pas encore d'évaluation
- Chapter 6 - Dimension of Development - Health AwarenessDocument12 pagesChapter 6 - Dimension of Development - Health AwarenessAsh MoorePas encore d'évaluation
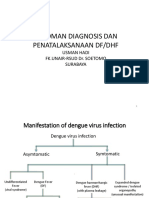
- DHF - DinkesDocument31 pagesDHF - DinkesAlfindraHaidaNabilaPas encore d'évaluation
- GROUP 5 FINAL RESEARCH PAPER - Docx 2Document14 pagesGROUP 5 FINAL RESEARCH PAPER - Docx 2af.026010Pas encore d'évaluation
- Dengue Update - As of Aug. 9, 2019Document10 pagesDengue Update - As of Aug. 9, 2019CHICKYPas encore d'évaluation
- CHAPTER-1 Citrus MaximaDocument5 pagesCHAPTER-1 Citrus MaximaSarah VillaPas encore d'évaluation
- Pathophysiology Dengue 2Document4 pagesPathophysiology Dengue 2KatherinePas encore d'évaluation
- Tropical Diseases An Unsolved ChallengeDocument9 pagesTropical Diseases An Unsolved ChallengeYet Barreda BasbasPas encore d'évaluation
- Vector Borne DiseasesDocument23 pagesVector Borne DiseasesKanishk BhatiaPas encore d'évaluation
- PapayaDocument6 pagesPapayaSaya SufiaPas encore d'évaluation
- MBI Questionaire UrduDocument6 pagesMBI Questionaire UrduMuhammad Zeeshan AaqibPas encore d'évaluation
- 2016-Biji Annona Muricara SoursopDocument11 pages2016-Biji Annona Muricara SoursopDwiPas encore d'évaluation
- PM1ch21 ARTHROPODS OF MILITARY IMPORTANCEDocument35 pagesPM1ch21 ARTHROPODS OF MILITARY IMPORTANCELee SmithPas encore d'évaluation
- Larvicidal Potential of AtisDocument17 pagesLarvicidal Potential of AtisKALUGDAN, Luis Gabriel, S.Pas encore d'évaluation
- Dengue ParasitologyDocument5 pagesDengue ParasitologyMadhav SorathiaPas encore d'évaluation
- Case Study: (Dengue Fever) Prepared byDocument9 pagesCase Study: (Dengue Fever) Prepared byMelody B. MiguelPas encore d'évaluation
- The Efficacy of Allium Sativum With Eucalyptus Globulus (Alleu) Teabag in Repelling Aedes AegyptiDocument20 pagesThe Efficacy of Allium Sativum With Eucalyptus Globulus (Alleu) Teabag in Repelling Aedes AegyptiSarah Candelaria ArcellanaPas encore d'évaluation
- A Rbo VirusesDocument2 pagesA Rbo VirusesDapoy PeraltaPas encore d'évaluation
- Mosquito Repellent Finish of Cotton Fabric by Extracting Castor OilDocument6 pagesMosquito Repellent Finish of Cotton Fabric by Extracting Castor OilTRUSHA PITHADIYAPas encore d'évaluation
- Arif 2009Document2 pagesArif 2009FihzanPas encore d'évaluation
- Criteria Computation Actual Score Justification 1. Nature of The ProblemDocument8 pagesCriteria Computation Actual Score Justification 1. Nature of The ProblemChin Villanueva UlamPas encore d'évaluation
- Dengue FormDocument2 pagesDengue FormZurc Saquin ApepePas encore d'évaluation
- What Is Dengue?: The VirusDocument1 pageWhat Is Dengue?: The VirusRogie SaludoPas encore d'évaluation