Vous aimerez peut-être aussi
- Occlusion and Splint Therapy: Tooth Surface LossDocument6 pagesOcclusion and Splint Therapy: Tooth Surface LossAdina SerbanPas encore d'évaluation
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahPas encore d'évaluation
- Ellinger 1971Document7 pagesEllinger 1971Mohammed TarekPas encore d'évaluation
- Orth Update 2023 16 85-90Document6 pagesOrth Update 2023 16 85-90jlkdsjfljsdlfPas encore d'évaluation
- Gingival Replacement in The Aesthetic ZoneDocument6 pagesGingival Replacement in The Aesthetic ZoneLynda M. NaranjoPas encore d'évaluation
- Ridge Preservation/Decoronation: Barbro Malmgren, DDS, PHDDocument6 pagesRidge Preservation/Decoronation: Barbro Malmgren, DDS, PHDMagPas encore d'évaluation
- Occlusion and Removable ProsthodonticsDocument8 pagesOcclusion and Removable ProsthodonticsMarylin AngPas encore d'évaluation
- 10VDocument10 pages10VValentina Paz Torres SepúlvedaPas encore d'évaluation
- Sauser 1957Document9 pagesSauser 1957Sahana RangarajanPas encore d'évaluation
- Avulsed Maxillary Central Incisors: The Case For ReplantationDocument5 pagesAvulsed Maxillary Central Incisors: The Case For ReplantationJessie PcdPas encore d'évaluation
- Molar Intrusion Using TADsDocument7 pagesMolar Intrusion Using TADsDr. Neesu KumbhatPas encore d'évaluation
- Milton Lappin, Detroit, MichDocument10 pagesMilton Lappin, Detroit, MichMarcos CastroPas encore d'évaluation
- The Monoplane Occlusion For Complete Dentures: T H e SP Herical TheoryDocument7 pagesThe Monoplane Occlusion For Complete Dentures: T H e SP Herical TheorySahana RangarajanPas encore d'évaluation
- Zachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationDocument5 pagesZachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationplsssssPas encore d'évaluation
- Determining Replacement Teeth Position For The Implant-Retained Prosthesis in The Edentulous PatientDocument8 pagesDetermining Replacement Teeth Position For The Implant-Retained Prosthesis in The Edentulous PatientTiago SpeziaPas encore d'évaluation
- Dental Update 2010. Consequences of Tooth Loss 2. Dentist Considerations Restorative Problems and ImplicationsDocument5 pagesDental Update 2010. Consequences of Tooth Loss 2. Dentist Considerations Restorative Problems and ImplicationsJay PatelPas encore d'évaluation
- The Great Occlusion Fiasco: DitorialDocument2 pagesThe Great Occlusion Fiasco: DitorialruacondungmanhPas encore d'évaluation
- ملخصDocument11 pagesملخصhgfdsPas encore d'évaluation
- CrossBite Lecture Dr. Hadeel AdelDocument10 pagesCrossBite Lecture Dr. Hadeel Adelعمار سعدPas encore d'évaluation
- Mandibular Incisor Extraction TherapyDocument10 pagesMandibular Incisor Extraction TherapyLeonardo LamimPas encore d'évaluation
- Dimension VerticalDocument17 pagesDimension Verticalger moralesPas encore d'évaluation
- Occlusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsDocument16 pagesOcclusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsHector Flores Soto100% (4)
- DT DEC 15 Germain FNLDocument10 pagesDT DEC 15 Germain FNLKranti PrajapatiPas encore d'évaluation
- 3 Single CDDocument7 pages3 Single CDdrgayen6042Pas encore d'évaluation
- Dahl ConceptDocument3 pagesDahl ConceptmusaabsiddiquiPas encore d'évaluation
- Single Complete Denture FinalDocument15 pagesSingle Complete Denture FinalVikas AggarwalPas encore d'évaluation
- 2 Registration Stage 2Document6 pages2 Registration Stage 2barbiePas encore d'évaluation
- Abfraction Lesions Reviewed: Current Concepts: Revisão - ReviewDocument6 pagesAbfraction Lesions Reviewed: Current Concepts: Revisão - ReviewdalipraiPas encore d'évaluation
- Point of CareDocument6 pagesPoint of Carepbo4Pas encore d'évaluation
- Vertical Control With TADs: Procedures and ProtocolsDocument15 pagesVertical Control With TADs: Procedures and ProtocolsCynthia AlfaroPas encore d'évaluation
- Prosthodontic Rehabilitation With Onlay Removable Partial Denture: A CaseDocument6 pagesProsthodontic Rehabilitation With Onlay Removable Partial Denture: A CasedjianPas encore d'évaluation
- The Space-Closure Alternative For Missing Maxillary Lateral Incisors: An UpdateDocument11 pagesThe Space-Closure Alternative For Missing Maxillary Lateral Incisors: An UpdateAbdelhamid MohamedPas encore d'évaluation
- Hudson Ling Arch 2013Document6 pagesHudson Ling Arch 2013Manda JoanPas encore d'évaluation
- 1964 Lawrence A. WeinbergDocument13 pages1964 Lawrence A. Weinberg謎超人Pas encore d'évaluation
- A Longitudinal Evaluation of Extraction Versus Nonextraction Treatment With Special Reference To The Posttreatment Irregularity of The Lower IncisorsDocument11 pagesA Longitudinal Evaluation of Extraction Versus Nonextraction Treatment With Special Reference To The Posttreatment Irregularity of The Lower IncisorsBeatriz ChilenoPas encore d'évaluation
- Correction of Anterior Dental Crossbite With Composite As An Inclined PlaneDocument8 pagesCorrection of Anterior Dental Crossbite With Composite As An Inclined PlaneALEJANDRA INÉS NIETO ARIASPas encore d'évaluation
- Functional OcclusionDocument9 pagesFunctional Occlusionvarsha palledPas encore d'évaluation
- J Esthet Restor Dent 2007 Vence-1Document7 pagesJ Esthet Restor Dent 2007 Vence-1MairaMaraviChavezPas encore d'évaluation
- How To Effectively Use A 264 Appliance: Features SectionDocument11 pagesHow To Effectively Use A 264 Appliance: Features SectionYerly Ramirez MuñozPas encore d'évaluation
- Chapter 2: Operative Dentistry and Prosthodontics: AnswersDocument13 pagesChapter 2: Operative Dentistry and Prosthodontics: AnswersBinayak UpadhyayaPas encore d'évaluation
- 3Document17 pages3paula catanaPas encore d'évaluation
- Space LossDocument5 pagesSpace LossAsma NawazPas encore d'évaluation
- Dahl ApplianceDocument8 pagesDahl Appliancesarah wilderPas encore d'évaluation
- 6+SADJ June 2022 Review Part+5+New+roots+titanium+and+its+influenceDocument5 pages6+SADJ June 2022 Review Part+5+New+roots+titanium+and+its+influenceDr. Zardasht N. BradostyPas encore d'évaluation
- When Does A Patient Need A "Functional Analysis" of Their Dental Occlusion?Document3 pagesWhen Does A Patient Need A "Functional Analysis" of Their Dental Occlusion?David ColonPas encore d'évaluation
- Vertical Ridge Augmentation and Soft Tissue Reconstruction of The Anterior Atrophic Maxillae - Urban2017Document12 pagesVertical Ridge Augmentation and Soft Tissue Reconstruction of The Anterior Atrophic Maxillae - Urban2017Claudio GuzmanPas encore d'évaluation
- Reviewing The Concept of Dahl: S S A J. SDocument5 pagesReviewing The Concept of Dahl: S S A J. Spablogdv956Pas encore d'évaluation
- Single Complete DentureDocument12 pagesSingle Complete DentureHarsha Reddy100% (1)
- Lingualized Occlusion ReviewDocument3 pagesLingualized Occlusion ReviewJessy ChenPas encore d'évaluation
- Boucher1944Document8 pagesBoucher1944luis sanchezPas encore d'évaluation
- Curve of Spee 2018Document7 pagesCurve of Spee 2018Thendral DevanathanPas encore d'évaluation
- Surgery As An Aid To More Efficient Service With Prosthetic Dentures KazanjianDocument16 pagesSurgery As An Aid To More Efficient Service With Prosthetic Dentures KazanjianJuan Sierra ZambranoPas encore d'évaluation
- Mordida Aberta 2Document7 pagesMordida Aberta 2Mariane Souza PintoPas encore d'évaluation
- Answer Key For Sample Examination: EndodonticsDocument4 pagesAnswer Key For Sample Examination: EndodonticsBinayak UpadhyayaPas encore d'évaluation
- Esthetic Noncarious Class V Restorations: A Case ReportDocument10 pagesEsthetic Noncarious Class V Restorations: A Case ReporttsukiyaPas encore d'évaluation
- Burke Et Al-2009-Journal of Esthetic and Restorative DentistryDocument4 pagesBurke Et Al-2009-Journal of Esthetic and Restorative DentistryMatheus CostaPas encore d'évaluation
- Relining Complete DentureDocument14 pagesRelining Complete DenturesasanPas encore d'évaluation
- Articulo Luis Diaz 2014Document8 pagesArticulo Luis Diaz 2014Andres CoboPas encore d'évaluation
- Registration: Stage II - Intermaxillary Relations: ProstheticsDocument6 pagesRegistration: Stage II - Intermaxillary Relations: ProstheticsOmar RamadanPas encore d'évaluation
- DfsdfsDocument12 pagesDfsdfsSitiKhadijahPas encore d'évaluation
- Review Article: A New Classification of Endodontic-Periodontal LesionsDocument6 pagesReview Article: A New Classification of Endodontic-Periodontal LesionsSitiKhadijahPas encore d'évaluation
- X-Smart Plus Brochure Maillefer Badge enDocument3 pagesX-Smart Plus Brochure Maillefer Badge enSitiKhadijahPas encore d'évaluation
- 2004 EndodtopicsHaapasaloetal PDFDocument28 pages2004 EndodtopicsHaapasaloetal PDFSitiKhadijahPas encore d'évaluation
- Postgraduate Department of Conservative Dentistry and EndodonticsDocument125 pagesPostgraduate Department of Conservative Dentistry and EndodonticsSitiKhadijahPas encore d'évaluation
- BDA Occlusion Seminar 2Document88 pagesBDA Occlusion Seminar 2SitiKhadijahPas encore d'évaluation
- Gurrea Bruguera IJED 2014Document18 pagesGurrea Bruguera IJED 2014SitiKhadijahPas encore d'évaluation
- Implant-Retained Cantilever Fixed Prosthesis: Where and WhenDocument4 pagesImplant-Retained Cantilever Fixed Prosthesis: Where and WhenSitiKhadijahPas encore d'évaluation
- Mixed Designs: Between and Within: Psy 420 AinsworthDocument30 pagesMixed Designs: Between and Within: Psy 420 AinsworthSitiKhadijahPas encore d'évaluation
- 11 SPSS Procedure For Kruskal Wallis TestDocument5 pages11 SPSS Procedure For Kruskal Wallis TestSitiKhadijahPas encore d'évaluation
- The Relationship Between Dentin Microhardness and Tubule DensityDocument5 pagesThe Relationship Between Dentin Microhardness and Tubule DensitySitiKhadijahPas encore d'évaluation
- The Hybrid Denture1Document9 pagesThe Hybrid Denture1SitiKhadijah100% (1)
- Bedrossian Treatment Planning The Maxilla PDFDocument11 pagesBedrossian Treatment Planning The Maxilla PDFSitiKhadijahPas encore d'évaluation
- Arts 9 M1 Q3 1Document15 pagesArts 9 M1 Q3 1Gina GalvezPas encore d'évaluation
- Self Regulatory Games For ChildrenDocument5 pagesSelf Regulatory Games For ChildrenKIP-HIDRAULIKA MPas encore d'évaluation
- Talking About Special Occasions American English StudentDocument5 pagesTalking About Special Occasions American English Studentmarinewuser8Pas encore d'évaluation
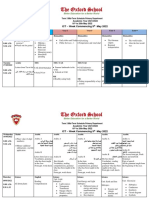
- Term 3 Mid-Term Assessment ScheduleDocument9 pagesTerm 3 Mid-Term Assessment ScheduleRabia MoeedPas encore d'évaluation
- Types of Editorial Texts: Queen Zayra Dela Rosa Francisco DagohoyDocument8 pagesTypes of Editorial Texts: Queen Zayra Dela Rosa Francisco DagohoyAkiro KaitoPas encore d'évaluation
- Cs6109 - Compiler Design: Lab AssignmentDocument8 pagesCs6109 - Compiler Design: Lab AssignmentvezhaventhanPas encore d'évaluation
- Strucni TekstDocument6 pagesStrucni TekstDusanPas encore d'évaluation
- Youcastr Case StudyDocument2 pagesYoucastr Case StudyMomina NadeemPas encore d'évaluation
- A Comprehensive Study of Types of Conditionals in LinguisticsDocument4 pagesA Comprehensive Study of Types of Conditionals in LinguisticsRyan CortezPas encore d'évaluation
- Mission: Children'SDocument36 pagesMission: Children'SWillian A. Palacio MurilloPas encore d'évaluation
- Lost On Mystery Mountain - The Ghost (PG 3&4)Document52 pagesLost On Mystery Mountain - The Ghost (PG 3&4)Olivia LeePas encore d'évaluation
- Different Types of Speeches According To DeliveryDocument18 pagesDifferent Types of Speeches According To DeliveryJoy Agustin100% (1)
- Week 1 Reading 2Document35 pagesWeek 1 Reading 2Prakhar ManasPas encore d'évaluation
- Business Cycle PDFDocument15 pagesBusiness Cycle PDFBernard OkpePas encore d'évaluation
- 99 Attributes of Allah Al Khaliq (The Creator) Al Bari (The Inventor) Al Musawwir (The Fashioner)Document7 pages99 Attributes of Allah Al Khaliq (The Creator) Al Bari (The Inventor) Al Musawwir (The Fashioner)Abdourahamane GarbaPas encore d'évaluation
- Role of Communication in BusinessDocument3 pagesRole of Communication in Businessmadhu motkur100% (2)
- Schema and Reading Comprehension Relative To Academic Performance of Grade 10 Students at Binulasan Integrated SchoolDocument12 pagesSchema and Reading Comprehension Relative To Academic Performance of Grade 10 Students at Binulasan Integrated SchoolShenly EchemanePas encore d'évaluation
- VocabularyDocument7 pagesVocabularyReynald Satria Dwiky IrawanPas encore d'évaluation
- Aub Updated-1 PDFDocument87 pagesAub Updated-1 PDFEvelyn Pamela Espinoza Morales100% (2)
- Usher Hall, Edinburgh: HistoryDocument1 pageUsher Hall, Edinburgh: HistoryTarun TangoPas encore d'évaluation
- The Body Shop Marketing Plan AnalysisDocument18 pagesThe Body Shop Marketing Plan AnalysisHepita0% (1)
- 125) League of Cities of The Philippines vs. COMELEC (G.R. No. 176951, April 12, 2011) 2Document35 pages125) League of Cities of The Philippines vs. COMELEC (G.R. No. 176951, April 12, 2011) 2Carmel Grace KiwasPas encore d'évaluation
- TRAFFIC JUNCTION SIMULATION-projectDocument45 pagesTRAFFIC JUNCTION SIMULATION-projectmacklyn tyan100% (2)
- Sample Legal Advice Problems and AnswersDocument4 pagesSample Legal Advice Problems and AnswersJake Bryson DancelPas encore d'évaluation
- Subject: Managerial Accounting Topic: Total Quality Management Reporter: Romalyn R. PurificacionDocument2 pagesSubject: Managerial Accounting Topic: Total Quality Management Reporter: Romalyn R. Purificacionromalyn purificacionPas encore d'évaluation
- Life and Work of Architect Ejaz AhedDocument25 pagesLife and Work of Architect Ejaz Ahedwajihazahid100% (2)
- How To Reset AutoCAD To Defaults - AutoCAD 2019 - Autodesk Knowledge NetworkDocument11 pagesHow To Reset AutoCAD To Defaults - AutoCAD 2019 - Autodesk Knowledge NetworkZina MorPas encore d'évaluation
- Giving Counsel PDFDocument42 pagesGiving Counsel PDFPaul ChungPas encore d'évaluation
- Ijel - Mickey's Christmas Carol A Derivation That IDocument6 pagesIjel - Mickey's Christmas Carol A Derivation That ITJPRC PublicationsPas encore d'évaluation
- Performance AnalyticsDocument193 pagesPerformance AnalyticsGPas encore d'évaluation