Vous aimerez peut-être aussi
- Neurological Observation Chart A3 Spreads - Layout 1Document2 pagesNeurological Observation Chart A3 Spreads - Layout 1Arun C RajPas encore d'évaluation
- Fbrmar: BrteresDocument11 pagesFbrmar: BrteresKaren Sofía Lucas FrancoPas encore d'évaluation
- Complete Cellist - Rudolf MatzDocument163 pagesComplete Cellist - Rudolf Matzevans_pritchard100% (2)
- KloqueDocument2 pagesKloquehumildejesus119Pas encore d'évaluation
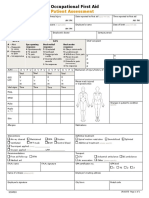
- TGL/HP Subjektif Objektif Ass + Ct/Mri/Lab PlanDocument2 pagesTGL/HP Subjektif Objektif Ass + Ct/Mri/Lab PlanRifqi MuhammadPas encore d'évaluation
- HNNE Complete 12 - 6 - 17Document3 pagesHNNE Complete 12 - 6 - 17Dr. Nirbhay MehtaPas encore d'évaluation
- HNNE Term Proforma Front Sheet 2008 With InstructionsDocument4 pagesHNNE Term Proforma Front Sheet 2008 With InstructionsMaribel MuevecelaPas encore d'évaluation
- Hip FractureDocument3 pagesHip Fracturenursing concept mapsPas encore d'évaluation
- 55m60 PDF enDocument1 page55m60 PDF enPSPas encore d'évaluation
- Aritmije BoronDocument1 pageAritmije BoronKristijan GoldašićPas encore d'évaluation
- Abbreviations 1Document8 pagesAbbreviations 1Rhona Marie AcuñaPas encore d'évaluation
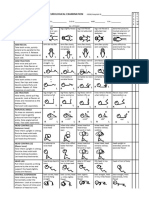
- Cervical Spine Physical ExamDocument1 pageCervical Spine Physical ExamEsther BPas encore d'évaluation
- CubeHead PLL 1.1Document9 pagesCubeHead PLL 1.1Steve PaimaPas encore d'évaluation
- Ini Al Evalua On/plan of Care - 6/27/2019: AssessmentDocument2 pagesIni Al Evalua On/plan of Care - 6/27/2019: AssessmentlizPas encore d'évaluation
- Javma-Javma 21 01 0013Document4 pagesJavma-Javma 21 01 0013Fiorella YavarPas encore d'évaluation
- 施儀謙 神經 chart書面Document7 pages施儀謙 神經 chart書面林良駿Pas encore d'évaluation
- Saunders Q&A ReviewDocument368 pagesSaunders Q&A ReviewDeepakPas encore d'évaluation
- Full Spine ListingsDocument3 pagesFull Spine ListingsMatthew DriscollPas encore d'évaluation
- Positioning TableDocument12 pagesPositioning TableJonathanPas encore d'évaluation
- Balance Notes PDFDocument4 pagesBalance Notes PDFFarhan Ullah KhanPas encore d'évaluation
- Haplik b2Document2 pagesHaplik b2Clint Mikael EulatrizPas encore d'évaluation
- Objectives To Find Compositions of Isometries, Including Glide ReflectionsDocument7 pagesObjectives To Find Compositions of Isometries, Including Glide ReflectionsAbood SafadiPas encore d'évaluation
- (Physio A) ECG (Javier)Document4 pages(Physio A) ECG (Javier)AliPas encore d'évaluation
- MSK AssessmentDocument5 pagesMSK AssessmentJacobs physcialtherapyPas encore d'évaluation
- AbbreviationsDocument9 pagesAbbreviationsYuuki Chitose (tai-kun)Pas encore d'évaluation
- Posi Appendicular Table NotesDocument12 pagesPosi Appendicular Table NotesAngelica Montalbo Nava100% (1)
- Sports Officiating: A. Basketball Hand SignalsDocument4 pagesSports Officiating: A. Basketball Hand SignalsStephanie DagohoyPas encore d'évaluation
- Sports Officiating Hand Signal RepairedDocument4 pagesSports Officiating Hand Signal RepairedJohn Lawrence ZabalaPas encore d'évaluation
- Cubehead'S PLL Algs: The Complete Alg-Sheet To Learn PLL As A WholeDocument9 pagesCubehead'S PLL Algs: The Complete Alg-Sheet To Learn PLL As A WholeLmao80% (5)
- Neuro PE Cheat SheetDocument2 pagesNeuro PE Cheat SheetJill Sanchez-SadiaPas encore d'évaluation
- AbbreviationsDocument9 pagesAbbreviationsZyra SantosPas encore d'évaluation
- AbbreviationsDocument9 pagesAbbreviationsZyra SantosPas encore d'évaluation
- Social Dances and Dance Mixers: Introductory ConceptDocument9 pagesSocial Dances and Dance Mixers: Introductory ConceptJay R BellenPas encore d'évaluation
- Prescription Abbreviations Used in PharmacyDocument2 pagesPrescription Abbreviations Used in PharmacySolCharmerPas encore d'évaluation
- Positioning-QuestionsDocument30 pagesPositioning-QuestionsAdrianne Jane Relova100% (1)
- Neurotype 1B-Strength & Power - v1Document18 pagesNeurotype 1B-Strength & Power - v1Lucas Toxopeus100% (4)
- Neurological Assessment Monitoring Sheet: C O M ADocument2 pagesNeurological Assessment Monitoring Sheet: C O M AAina HaravataPas encore d'évaluation
- Potential Transformers: AB ACDocument5 pagesPotential Transformers: AB ACsahale sheraPas encore d'évaluation
- Josh's Megaminx GuideDocument1 pageJosh's Megaminx GuideBoris IvanovPas encore d'évaluation
- FIBA Officiating SignalsDocument6 pagesFIBA Officiating SignalsAhle MaePas encore d'évaluation
- FIBA Officiating SignalsDocument6 pagesFIBA Officiating SignalsSophia Lorin TemcangPas encore d'évaluation
- Profile Assessment Profile Assessment: Leonardo MurabitoDocument26 pagesProfile Assessment Profile Assessment: Leonardo Murabito冷腾Pas encore d'évaluation
- Gray Institute Work SheetsDocument39 pagesGray Institute Work Sheetskokoliu liu100% (2)
- Jayme MV Dance TerminologiesDocument8 pagesJayme MV Dance TerminologiesMaxine JaymePas encore d'évaluation
- Carinosa (The National Dance of The Philippines) : Formation: PointingDocument4 pagesCarinosa (The National Dance of The Philippines) : Formation: PointingFiona SalacyaoPas encore d'évaluation
- Mtv15.0 PT Postureassessment 160609 v1.0Document2 pagesMtv15.0 PT Postureassessment 160609 v1.0tommy58Pas encore d'évaluation
- Postural AssessmentDocument2 pagesPostural AssessmentKedar KelkarPas encore d'évaluation
- Stockard Tests UE & LE TDocument4 pagesStockard Tests UE & LE TLinh HoangPas encore d'évaluation
- PHC Ankle SprainDocument5 pagesPHC Ankle SprainMin WajePas encore d'évaluation
- Southeast Veterinary Neurology Neurologic Exam Form: Patient Name: Age: Gender: BreedDocument2 pagesSoutheast Veterinary Neurology Neurologic Exam Form: Patient Name: Age: Gender: BreedAndres MartinezPas encore d'évaluation
- Hip Assessment Form Incl THA Revised October 2017Document2 pagesHip Assessment Form Incl THA Revised October 2017RishaadPas encore d'évaluation
- Chapitre I-2-: B - Associations de Dipôles Passifs LinéairesDocument2 pagesChapitre I-2-: B - Associations de Dipôles Passifs LinéairesFth Walter100% (1)
- Indentificacion de Instrumentos FINALDocument13 pagesIndentificacion de Instrumentos FINALEdward GarciaPas encore d'évaluation
- Adobe Scan 26 Nov 2021Document12 pagesAdobe Scan 26 Nov 2021Pallabi dePas encore d'évaluation
- Medical Pharmacy Abbreviation PDFDocument5 pagesMedical Pharmacy Abbreviation PDFANJALI RAJBHARPas encore d'évaluation
- Table 1. Latin Abbreviations Partial List of Prescription Abbreviations Abbreviation Latin MeaningDocument6 pagesTable 1. Latin Abbreviations Partial List of Prescription Abbreviations Abbreviation Latin MeaningFathoni EnggartyastaPas encore d'évaluation
- Chapter 4 l2Document7 pagesChapter 4 l2Rommel Samonte AlonzagayPas encore d'évaluation
- Harpistsdailydoz 01 SalzDocument24 pagesHarpistsdailydoz 01 SalzalastanczPas encore d'évaluation
- Physiotherapy MOPDocument20 pagesPhysiotherapy MOPHbk RajneeshPas encore d'évaluation
- Resume Alok (M.P.T.)Document3 pagesResume Alok (M.P.T.)Hbk RajneeshPas encore d'évaluation
- Positioning Techniques in Long-Term Care: Self-Directed Learning Package For Health Care ProvidersDocument41 pagesPositioning Techniques in Long-Term Care: Self-Directed Learning Package For Health Care ProvidersHbk RajneeshPas encore d'évaluation
- AmityDocument1 pageAmityHbk RajneeshPas encore d'évaluation
- Jospt 1984 5 6 348Document25 pagesJospt 1984 5 6 348Hbk RajneeshPas encore d'évaluation
- To Whom So Ever It May Concern RAJNEESH SUVIDHADocument1 pageTo Whom So Ever It May Concern RAJNEESH SUVIDHAHbk RajneeshPas encore d'évaluation
- New Microsoft Office Word DocumentDocument1 pageNew Microsoft Office Word DocumentHbk RajneeshPas encore d'évaluation
- Internship Certificate KalpanaDocument1 pageInternship Certificate KalpanaHbk Rajneesh0% (1)
- SSC Coo RRPP..CC Oom M: Ssa Am MPP LleeDocument2 pagesSSC Coo RRPP..CC Oom M: Ssa Am MPP LleeHbk RajneeshPas encore d'évaluation
- Cghs List: Department of Physiotherapy MonthDocument1 pageCghs List: Department of Physiotherapy MonthHbk RajneeshPas encore d'évaluation
- Internship CertificateDocument1 pageInternship CertificateHbk Rajneesh80% (5)
- 3507P 11Document2 pages3507P 11Hbk RajneeshPas encore d'évaluation
- Physiotherapy Department: Anant HospitalDocument1 pagePhysiotherapy Department: Anant HospitalHbk RajneeshPas encore d'évaluation
- Group Members Topic Date: Pt-Iii Group Presentation BPT Final YearDocument1 pageGroup Members Topic Date: Pt-Iii Group Presentation BPT Final YearHbk RajneeshPas encore d'évaluation
- These DiscussionDocument7 pagesThese DiscussionHbk RajneeshPas encore d'évaluation
- PDF SampleDocument1 pagePDF SamplejoauraPas encore d'évaluation
- Common Special TestsDocument6 pagesCommon Special Testsramesh_chbptPas encore d'évaluation
- Surgery SyllabusDocument1 pageSurgery SyllabusHbk RajneeshPas encore d'évaluation
- 09 2566Document20 pages09 2566Hbk RajneeshPas encore d'évaluation
- Muscle StimulatorDocument1 pageMuscle StimulatorHbk RajneeshPas encore d'évaluation
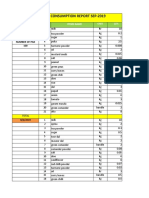
- Daily Staff Food Consumption Reports Sep-2019Document4 pagesDaily Staff Food Consumption Reports Sep-2019Manjit RawatPas encore d'évaluation
- E61 DiagramDocument79 pagesE61 Diagramthanes1027Pas encore d'évaluation
- 1A Wound Care AdviceDocument2 pages1A Wound Care AdviceGrace ValenciaPas encore d'évaluation
- Solo ParentsDocument1 pageSolo ParentsOZ CincoPas encore d'évaluation
- PEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesDocument2 pagesPEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesLady Diana TiangcoPas encore d'évaluation
- Iomm VFD-3 030112Document100 pagesIomm VFD-3 030112Alexander100% (1)
- Biochem Nucleic Acid ReviewerDocument5 pagesBiochem Nucleic Acid ReviewerGabrielle FranciscoPas encore d'évaluation
- Characteristics of Testable HypothesesDocument30 pagesCharacteristics of Testable HypothesesMarivic Diano67% (3)
- CONTROLTUB - Controle de Juntas - New-Flare-Piping-Joints-ControlDocument109 pagesCONTROLTUB - Controle de Juntas - New-Flare-Piping-Joints-ControlVss SantosPas encore d'évaluation
- Heart Sounds: Presented by Group 2A & 3ADocument13 pagesHeart Sounds: Presented by Group 2A & 3AMeow Catto100% (1)
- Valve Material SpecificationDocument397 pagesValve Material Specificationkaruna34680% (5)
- Phardose Lab Prep 19 30Document4 pagesPhardose Lab Prep 19 30POMPEYO BARROGAPas encore d'évaluation
- Notes Marriage and Family in Canon LawDocument5 pagesNotes Marriage and Family in Canon LawmacPas encore d'évaluation
- Recruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFDocument7 pagesRecruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFSneha KadamPas encore d'évaluation
- HUM110 Gilgamesh EssayDocument4 pagesHUM110 Gilgamesh EssaynsmeganPas encore d'évaluation
- Plica PDFDocument7 pagesPlica PDFIVAN VERGARAPas encore d'évaluation
- Electri RelifDocument18 pagesElectri Relifsuleman247Pas encore d'évaluation
- Comparative Pharmacology For AnesthetistDocument162 pagesComparative Pharmacology For AnesthetistGayatri PalacherlaPas encore d'évaluation
- Cargador de BateríaDocument34 pagesCargador de BateríaBenPas encore d'évaluation
- Introduction and Vapour Compression CycleDocument29 pagesIntroduction and Vapour Compression Cycleمحسن الراشدPas encore d'évaluation
- Carboset CA-600 - CST600 - CO - enDocument3 pagesCarboset CA-600 - CST600 - CO - enNilsPas encore d'évaluation
- Electrical Data: PD2310 ApplicationsDocument1 pageElectrical Data: PD2310 ApplicationsKSPas encore d'évaluation
- Epo-Fix Plus: High-Performance Epoxy Chemical AnchorDocument3 pagesEpo-Fix Plus: High-Performance Epoxy Chemical Anchormilivoj ilibasicPas encore d'évaluation
- TraceGains Inspection Day FDA Audit ChecklistDocument2 pagesTraceGains Inspection Day FDA Audit Checklistdrs_mdu48Pas encore d'évaluation
- Report in Per Dev CorrectedDocument34 pagesReport in Per Dev CorrectedJosh lyan RiveraPas encore d'évaluation
- How To Import Medical Devices Into The USDocument16 pagesHow To Import Medical Devices Into The USliviustitusPas encore d'évaluation
- The Vapour Compression Cycle (Sample Problems)Document3 pagesThe Vapour Compression Cycle (Sample Problems)allovid33% (3)
- 2005 Harley Davidson Sportster 883 66418Document136 pages2005 Harley Davidson Sportster 883 66418Josef Bruno SchlittenbauerPas encore d'évaluation
- Contractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountDocument1 pageContractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountusmanaliPas encore d'évaluation
- Neurocisticercosis PDFDocument7 pagesNeurocisticercosis PDFFiorella Alexandra HRPas encore d'évaluation