Vous aimerez peut-être aussi
- For Your Wedding: We Are You Perfect MatchDocument4 pagesFor Your Wedding: We Are You Perfect MatchFerry KusmalinggaPas encore d'évaluation
- Hookworm - Journal - 1 AchmadDocument8 pagesHookworm - Journal - 1 AchmadFerry KusmalinggaPas encore d'évaluation
- Pak Rusyad - AntropologiDocument34 pagesPak Rusyad - AntropologiFerry KusmalinggaPas encore d'évaluation
- Vclient LogDocument1 pageVclient LogFerry KusmalinggaPas encore d'évaluation
- Effect of Short Sleep Duration On Daily Activities - United States, 2005-2008Document5 pagesEffect of Short Sleep Duration On Daily Activities - United States, 2005-2008Ferry KusmalinggaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- OSADocument5 pagesOSAtherese BPas encore d'évaluation
- Guideline SummaryDocument9 pagesGuideline SummarymanmeetPas encore d'évaluation
- Neurological Disorders With Sleep Alterations: Cristina Panea, MD, PHD Elias Emergency University Hospital BucharestDocument20 pagesNeurological Disorders With Sleep Alterations: Cristina Panea, MD, PHD Elias Emergency University Hospital BucharestGrig GrigPas encore d'évaluation
- Why Do I Always Wake Up After 5 Hours of Sleep?Document35 pagesWhy Do I Always Wake Up After 5 Hours of Sleep?Joao MoreiraPas encore d'évaluation
- Portable Devices Used For Home Testing in Obstructive Sleep ApneaDocument42 pagesPortable Devices Used For Home Testing in Obstructive Sleep ApneaCalifornia Technology Assessment Forum0% (1)
- Signs and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeDocument7 pagesSigns and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeLuis De jesus SolanoPas encore d'évaluation
- Sleep Apnea Syndrome &Document28 pagesSleep Apnea Syndrome &Sumit PuloriaPas encore d'évaluation
- 2010 Philips Respironics CatalogDocument148 pages2010 Philips Respironics CatalogAcilegna BPas encore d'évaluation
- Practice Essentials: Ralph Downey, Iii, PHD Staff Sleep Specialist, Cleveland Clinic Foundation AssociateDocument18 pagesPractice Essentials: Ralph Downey, Iii, PHD Staff Sleep Specialist, Cleveland Clinic Foundation AssociateMaulana 'Sugat' Iskandar DinataPas encore d'évaluation
- Sleep Disorders in Myopathy 3.10.19Document16 pagesSleep Disorders in Myopathy 3.10.19Nitesh DahiyaPas encore d'évaluation
- By: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJDocument51 pagesBy: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJmeutiaputripuyPas encore d'évaluation
- SleepDocument8 pagesSleepDeepak GhanshalaPas encore d'évaluation
- Obstructive Sleep Apnea and Orthodontics: An American Association of Orthodontists White PaperDocument17 pagesObstructive Sleep Apnea and Orthodontics: An American Association of Orthodontists White PaperIsa TorresPas encore d'évaluation
- Prospekt BiPAP AutoDocument2 pagesProspekt BiPAP AutoADVANCE MICRONICSPas encore d'évaluation
- RespironicsDocument6 pagesRespironicsHuzur MezarPas encore d'évaluation
- Compact, Lightweight and Easy To Operate: Bipap S/TDocument2 pagesCompact, Lightweight and Easy To Operate: Bipap S/TMedSparkPas encore d'évaluation
- Postreading Self-Assessment and CME Test-Preferred ResponsesDocument10 pagesPostreading Self-Assessment and CME Test-Preferred Responsesdr.cidgutPas encore d'évaluation
- Effects of Occlusal Stabilization Splints On Obstructive Sleep Apnea A Randomized Controlled Trial PDFDocument7 pagesEffects of Occlusal Stabilization Splints On Obstructive Sleep Apnea A Randomized Controlled Trial PDFsemitsuPas encore d'évaluation
- Ventilator Waveforms DavidTuxen2Document41 pagesVentilator Waveforms DavidTuxen2Syed Shahrul Naz Syed100% (1)
- Abstract Book Appicon 2017Document242 pagesAbstract Book Appicon 2017Anil KumarPas encore d'évaluation
- Ferhm Effectiveness of Adenotonsillectomy Vs Watchful Waiting in Young ChildrenDocument17 pagesFerhm Effectiveness of Adenotonsillectomy Vs Watchful Waiting in Young Childrendanielesantos.202019Pas encore d'évaluation
- JRAM Volume 3 Issue 1 Pages 67-74Document8 pagesJRAM Volume 3 Issue 1 Pages 67-74Rehab BassamPas encore d'évaluation
- Sleep Medicine ReviewsDocument16 pagesSleep Medicine ReviewsCami ElenaPas encore d'évaluation
- PrintDocument65 pagesPrintLý TưởngPas encore d'évaluation
- Sleep Wake DisordersDocument68 pagesSleep Wake DisordersRashed ShatnawiPas encore d'évaluation
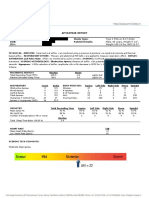
- Sample-Sleep Study Report PDFDocument2 pagesSample-Sleep Study Report PDFgopuPas encore d'évaluation
- Obstructive Sleep Apnoea and AnaesthesiaDocument21 pagesObstructive Sleep Apnoea and AnaesthesiajahangirealamPas encore d'évaluation
- Mullers Maneuver in Patients With Obstructive Sleep ApneaDocument4 pagesMullers Maneuver in Patients With Obstructive Sleep ApneaAji KusumaPas encore d'évaluation
- Risk Factors For Sleep-Disordered Breathing in Children: Associations With Obesity, Race, and Respiratory ProblemsDocument6 pagesRisk Factors For Sleep-Disordered Breathing in Children: Associations With Obesity, Race, and Respiratory ProblemsMiral BassPas encore d'évaluation
- Diagnosis and Treatment of Obstructive Sleep Apnea in AdultsDocument8 pagesDiagnosis and Treatment of Obstructive Sleep Apnea in AdultsTeuku Ilham AkbarPas encore d'évaluation