Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Honda CB450 K0 Parts List ManualDocument130 pagesHonda CB450 K0 Parts List ManualBrandon Parsons100% (1)
- PP - 3 Main Areas of A HouseDocument48 pagesPP - 3 Main Areas of A Houseapi-248930594Pas encore d'évaluation
- Employment Termination and Settlement AgreementDocument6 pagesEmployment Termination and Settlement AgreementParul KhannaPas encore d'évaluation
- Calalang Vs WilliamsDocument2 pagesCalalang Vs Williamsczabina fatima delicaPas encore d'évaluation
- Handout Cyberbully MovieDocument4 pagesHandout Cyberbully Movieapi-248930594Pas encore d'évaluation
- Romero V Estrada DigestDocument1 pageRomero V Estrada DigestPamela PrietoPas encore d'évaluation
- Crusades-Worksheet 2014Document2 pagesCrusades-Worksheet 2014api-263356428Pas encore d'évaluation
- The Forrester Wave PDFDocument15 pagesThe Forrester Wave PDFManish KumarPas encore d'évaluation
- Childrens Book Student ExampleDocument22 pagesChildrens Book Student Exampleapi-248930594Pas encore d'évaluation
- Release of Liability TransportationDocument1 pageRelease of Liability Transportationapi-248930594Pas encore d'évaluation
- My Educational PhilosophyDocument1 pageMy Educational Philosophyapi-248930594Pas encore d'évaluation
- Resume 2019Document1 pageResume 2019api-248930594Pas encore d'évaluation
- Robotics Contact 2Document1 pageRobotics Contact 2api-248930594Pas encore d'évaluation
- 2016 Fim Consent ReleaseDocument2 pages2016 Fim Consent Releaseapi-248930594Pas encore d'évaluation
- 2012-2013 Consent and Release FormDocument1 page2012-2013 Consent and Release FormTaide DingPas encore d'évaluation
- Parent Student AgreementDocument2 pagesParent Student Agreementapi-248930594Pas encore d'évaluation
- Budget Spreadsheet 2Document3 pagesBudget Spreadsheet 2api-248930594Pas encore d'évaluation
- Budget Spreadsheet 2Document3 pagesBudget Spreadsheet 2api-248930594Pas encore d'évaluation
- It 7150 Team Evaluation ProjectDocument15 pagesIt 7150 Team Evaluation Projectapi-248930594Pas encore d'évaluation
- Digital Communication Tools For The Classroom Educator: Professional Development Conference Leader GuideDocument8 pagesDigital Communication Tools For The Classroom Educator: Professional Development Conference Leader Guideapi-248930594Pas encore d'évaluation
- Food-Personal Expenses Spreadsheet 1Document1 pageFood-Personal Expenses Spreadsheet 1api-248930594Pas encore d'évaluation
- Investment Comparison Activity 9Document2 pagesInvestment Comparison Activity 9api-248930594Pas encore d'évaluation
- ISTE Nets-T StandardsDocument2 pagesISTE Nets-T StandardsjenniferkadienPas encore d'évaluation
- Final Build Project Evaluation Class EvalDocument3 pagesFinal Build Project Evaluation Class Evalapi-248930594Pas encore d'évaluation
- 15 1301 Architectural Drafting Consolidated Gap Analysis Final 1 B 1Document12 pages15 1301 Architectural Drafting Consolidated Gap Analysis Final 1 B 1api-248930594Pas encore d'évaluation
- Home Buying Project AlexDocument6 pagesHome Buying Project Alexapi-248930594Pas encore d'évaluation
- Chase Sample GuideDocument3 pagesChase Sample Guideapi-310599226Pas encore d'évaluation
- 20-14 Iste Standards-S PDFDocument2 pages20-14 Iste Standards-S PDFapi-189128099Pas encore d'évaluation
- 141 Furniture Arrangement and Traffic PatternsDocument20 pages141 Furniture Arrangement and Traffic Patternsapi-248930594Pas encore d'évaluation
- Group Members EvaluationDocument3 pagesGroup Members Evaluationapi-248930594Pas encore d'évaluation
- Final Evaluation Personal RubricDocument2 pagesFinal Evaluation Personal Rubricapi-248930594Pas encore d'évaluation
- Tips For TeensDocument1 pageTips For Teensapi-248930594Pas encore d'évaluation
- Youthengagement Brieftoolkit CompliantDocument4 pagesYouthengagement Brieftoolkit Compliantapi-248930594Pas encore d'évaluation
- Technology Use Contract 2014Document3 pagesTechnology Use Contract 2014api-248930594Pas encore d'évaluation
- Cyberbullying Flowchart 2015Document1 pageCyberbullying Flowchart 2015api-2489305940% (1)
- Rundo EmergencyDocument7 pagesRundo Emergency415timPas encore d'évaluation
- Two-Nation TheoryDocument6 pagesTwo-Nation TheoryAleeha IlyasPas encore d'évaluation
- PLM860SAW: Installation and Operation ManualDocument8 pagesPLM860SAW: Installation and Operation Manualjose angel guzman lozanoPas encore d'évaluation
- List of Officers Who Attended Courses at NCRB-2019Document189 pagesList of Officers Who Attended Courses at NCRB-2019Manish Bhardwaj100% (1)
- MIH International v. Comfortland MedicalDocument7 pagesMIH International v. Comfortland MedicalPriorSmartPas encore d'évaluation
- A Community For All: Looking at Our Common Caribbean Information HeritageDocument3 pagesA Community For All: Looking at Our Common Caribbean Information HeritageEmerson O. St. G. BryanPas encore d'évaluation
- 2011 CIVITAS Benefit JournalDocument40 pages2011 CIVITAS Benefit JournalCIVITASPas encore d'évaluation
- Criminal Punishment For Environmental DamageDocument25 pagesCriminal Punishment For Environmental DamagePatricio Castillo DoiziPas encore d'évaluation
- Annual Report 17-18Document96 pagesAnnual Report 17-18Sajib Chandra RoyPas encore d'évaluation
- Pre-Commencement Meeting and Start-Up ArrangementsDocument1 pagePre-Commencement Meeting and Start-Up ArrangementsGie SiegePas encore d'évaluation
- Understanding The 2007-2008 Global Financial Crisis: Lessons For Scholars of International Political EconomyDocument23 pagesUnderstanding The 2007-2008 Global Financial Crisis: Lessons For Scholars of International Political EconomyLeyla SaidPas encore d'évaluation
- Scott Gessler Appeal of Ethics Commission Sanctions - Opening BriefDocument56 pagesScott Gessler Appeal of Ethics Commission Sanctions - Opening BriefColorado Ethics WatchPas encore d'évaluation
- San Beda College Alabang Religious Education Department: Wounded FamiliesDocument13 pagesSan Beda College Alabang Religious Education Department: Wounded FamiliesHaydee FelicenPas encore d'évaluation
- AQA GCSE Citizenship Revision Guide - FINALDocument19 pagesAQA GCSE Citizenship Revision Guide - FINALJohn SmithPas encore d'évaluation
- Position Paper in Purposive CommunicationDocument2 pagesPosition Paper in Purposive CommunicationKhynjoan AlfilerPas encore d'évaluation
- Student Profile Guide G TuDocument5 pagesStudent Profile Guide G TuumeshPas encore d'évaluation
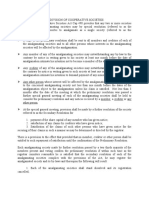
- Amalgamation of SocietiesDocument4 pagesAmalgamation of SocietiesKen ChepkwonyPas encore d'évaluation
- Windows 10 100% Disk Usage in Task Manager (SOLVED) - Driver EasyDocument46 pagesWindows 10 100% Disk Usage in Task Manager (SOLVED) - Driver EasyMrinal K MahatoPas encore d'évaluation
- Ultra 3000 Drive (2098-In003 - En-P)Document180 pagesUltra 3000 Drive (2098-In003 - En-P)Robert BarnettePas encore d'évaluation
- BeerVM11e PPT Ch11Document92 pagesBeerVM11e PPT Ch11brayanPas encore d'évaluation
- Bantolo V CastillonDocument3 pagesBantolo V Castillongoma21Pas encore d'évaluation
- FEE SCHEDULE 2017/2018: Cambridge IGCSE Curriculum Academic Year: August 2017 To July 2018Document1 pageFEE SCHEDULE 2017/2018: Cambridge IGCSE Curriculum Academic Year: August 2017 To July 2018anjanamenonPas encore d'évaluation
- Affidavit of UndertakingDocument3 pagesAffidavit of UndertakingPingotMagangaPas encore d'évaluation
- SAP Project System - A Ready Reference (Part 1) - SAP BlogsDocument17 pagesSAP Project System - A Ready Reference (Part 1) - SAP BlogsSUNIL palPas encore d'évaluation