Vous aimerez peut-être aussi
- Peds Derm 101 HH HandoutDocument25 pagesPeds Derm 101 HH HandoutzhuorancaiPas encore d'évaluation
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocument9 pagesYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliPas encore d'évaluation
- Hemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Acrodermatitis EnteropathicaDocument4 pagesAcrodermatitis EnteropathicaIntan FajrinPas encore d'évaluation
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
- PediatricsDocument38 pagesPediatricskhanPas encore d'évaluation
- Intertrigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandIntertrigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Teaching Diagnostic Error Using Problem-Based Learning: A Case of Cellulitis MisdiagnosisDocument4 pagesTeaching Diagnostic Error Using Problem-Based Learning: A Case of Cellulitis Misdiagnosisvadiningtyas3770Pas encore d'évaluation
- 7 Bleeding Disorders DR - AlaaDocument35 pages7 Bleeding Disorders DR - Alaaaj1998ajPas encore d'évaluation
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaD'EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaPas encore d'évaluation
- Scaling in DermatologyDocument4 pagesScaling in DermatologychandandojodePas encore d'évaluation
- Arensman 2nd 9781570597510Document499 pagesArensman 2nd 9781570597510Simina SerbanPas encore d'évaluation
- Problem-based Approach to Gastroenterology and HepatologyD'EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisPas encore d'évaluation
- Ve Siculo Bull Ous DiseasesDocument73 pagesVe Siculo Bull Ous DiseasesAARYAPas encore d'évaluation
- Guidelines For The Management of Nappy RashDocument13 pagesGuidelines For The Management of Nappy RashOva PradiptaPas encore d'évaluation
- Introduction To Dermatology Assessment of A Dermatologic PatientDocument86 pagesIntroduction To Dermatology Assessment of A Dermatologic PatientAtifPas encore d'évaluation
- Self Assessment CasesDocument512 pagesSelf Assessment CasesmixandgoPas encore d'évaluation
- Topical Antibiotics in DermatologyDocument19 pagesTopical Antibiotics in DermatologyJejem Marandra EmkamasPas encore d'évaluation
- New Concepts in the Management of Septic Perianal ConditionsD'EverandNew Concepts in the Management of Septic Perianal ConditionsPas encore d'évaluation
- Pediatric Blistering Diseases: MSU/Beaumont Health Dermatology Residency ProgramDocument80 pagesPediatric Blistering Diseases: MSU/Beaumont Health Dermatology Residency ProgramGeoRPas encore d'évaluation
- Dermnet NZ: Special Stains and TestsDocument4 pagesDermnet NZ: Special Stains and TestsRaja Sekaran DuraiPas encore d'évaluation
- Clinical Cases in Pigmentary DisordersD'EverandClinical Cases in Pigmentary DisordersTorello LottiPas encore d'évaluation
- Atopic Dermatitis 2013Document32 pagesAtopic Dermatitis 2013Bagus Maha ParadipaPas encore d'évaluation
- Molluscum Contagiosum Module - PPSXDocument38 pagesMolluscum Contagiosum Module - PPSXDevy Anggi SitompulPas encore d'évaluation
- Dermatology PDFDocument23 pagesDermatology PDFjonyPas encore d'évaluation
- Dermatology For The NonDermDocument7 pagesDermatology For The NonDermDaniellePas encore d'évaluation
- Melanocytic TumorsDocument170 pagesMelanocytic TumorsOlteanu Dragos-Nicolae100% (1)
- Sqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZDocument19 pagesSqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZkdwazirPas encore d'évaluation
- IPMdp 0801 A 12Document2 pagesIPMdp 0801 A 12Adelya AwdyaPas encore d'évaluation
- An Approach To The Patient With ErythrodermaDocument42 pagesAn Approach To The Patient With ErythrodermaShakilPas encore d'évaluation
- Practical Gastroenterology and Hepatology Board Review ToolkitD'EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultPas encore d'évaluation
- Dermatitis DR Citra 260907Document56 pagesDermatitis DR Citra 260907Adam AriwibawaPas encore d'évaluation
- 323 (1) - Angry Back - Excited Skin SyndromeDocument6 pages323 (1) - Angry Back - Excited Skin Syndromecohbipc100% (1)
- Technology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementD'EverandTechnology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementMichele FimianiPas encore d'évaluation
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2D'EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2Pas encore d'évaluation
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyD'EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyPas encore d'évaluation
- Wwa NodosumDocument21 pagesWwa NodosumMu AbPas encore d'évaluation
- Wieder SumDocument71 pagesWieder SumFlorin BujoreanuPas encore d'évaluation
- Clinical Cases in Dermatology Modern Management of Acne Actinic Keratosis and Atopic DermatitisDocument7 pagesClinical Cases in Dermatology Modern Management of Acne Actinic Keratosis and Atopic DermatitisJpratoPas encore d'évaluation
- Streptococcal PharyngitisDocument33 pagesStreptococcal PharyngitisIkrimaikPas encore d'évaluation
- Approach To A Patient of Bullous DisorderDocument50 pagesApproach To A Patient of Bullous DisorderAbhirut ThakurPas encore d'évaluation
- 10-4 Melanocytic LesionsDocument40 pages10-4 Melanocytic LesionsSorin DeacuPas encore d'évaluation
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- June 2022 - Dermatology - 10 McqsDocument8 pagesJune 2022 - Dermatology - 10 McqsAhmed ShihataPas encore d'évaluation
- Vesiculobullous Disorders in Children2Document5 pagesVesiculobullous Disorders in Children2Luciana FernandesPas encore d'évaluation
- Stevens-Johnson Syndrome (SJS)Document27 pagesStevens-Johnson Syndrome (SJS)Fitri wijayaPas encore d'évaluation
- Dermatology OSCE Pictures 1Document208 pagesDermatology OSCE Pictures 1medt80Pas encore d'évaluation
- 1993 92 723 Larry J. Baraff: Capillary Refill: Is It A Useful Clinical Sign?Document4 pages1993 92 723 Larry J. Baraff: Capillary Refill: Is It A Useful Clinical Sign?Citty'Q' HuwalidPas encore d'évaluation
- Clinical Profile of Acute Rheumatic Fever Patients Attending A Tertiary Care Hospital in Eastern Bihar, IndiaDocument4 pagesClinical Profile of Acute Rheumatic Fever Patients Attending A Tertiary Care Hospital in Eastern Bihar, IndiaraniaulfahPas encore d'évaluation
- Skin PDFDocument13 pagesSkin PDFLanaAmeriePas encore d'évaluation
- Chapter 116:: Melanoma:: Jessica C. Hassel & Alexander H. EnkDocument36 pagesChapter 116:: Melanoma:: Jessica C. Hassel & Alexander H. EnkJhauharina RfPas encore d'évaluation
- Suppurative KeratitisDocument30 pagesSuppurative KeratitisTatik Handayani100% (1)
- Steroid Pulse Therapies in DermatologyDocument4 pagesSteroid Pulse Therapies in DermatologyWelly WijayantiPas encore d'évaluation
- Jadwal Isip Igd Juli 2020Document4 pagesJadwal Isip Igd Juli 2020Tia AfelitaPas encore d'évaluation
- Spss PHDocument1 pageSpss PHTia AfelitaPas encore d'évaluation
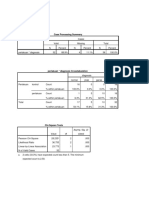
- Case Processing SummaryDocument2 pagesCase Processing SummaryTia AfelitaPas encore d'évaluation
- Presentasi: Evri Ekadiansyah, S. Kom., M. KomDocument19 pagesPresentasi: Evri Ekadiansyah, S. Kom., M. KomTia AfelitaPas encore d'évaluation
- Muslims' Contribution To Medicine: Dr. H. Elman Boy, M.Kes FK Umsu 2013Document36 pagesMuslims' Contribution To Medicine: Dr. H. Elman Boy, M.Kes FK Umsu 2013Tia AfelitaPas encore d'évaluation
- Hombres Mujeres Cmo Salir Del Camino Equivocado Spanish Edition by Badinter Lisabeth 950557584xDocument5 pagesHombres Mujeres Cmo Salir Del Camino Equivocado Spanish Edition by Badinter Lisabeth 950557584xFernanda Avilés CartagenaPas encore d'évaluation
- Klabin Reports 2nd Quarter Earnings of R$ 15 Million: HighlightsDocument10 pagesKlabin Reports 2nd Quarter Earnings of R$ 15 Million: HighlightsKlabin_RIPas encore d'évaluation
- Yukot,+houkelin 2505 11892735 Final+Paper+Group+41Document17 pagesYukot,+houkelin 2505 11892735 Final+Paper+Group+410191720003 ELIAS ANTONIO BELLO LEON ESTUDIANTE ACTIVOPas encore d'évaluation
- NCPDocument3 pagesNCPchesca_paunganPas encore d'évaluation
- E1979017519 PDFDocument7 pagesE1979017519 PDFAnant HatkamkarPas encore d'évaluation
- Types of Numbers: SeriesDocument13 pagesTypes of Numbers: SeriesAnonymous NhQAPh5toPas encore d'évaluation
- Julie Jacko - Professor of Healthcare InformaticsDocument1 pageJulie Jacko - Professor of Healthcare InformaticsjuliejackoPas encore d'évaluation
- Mathematics Paper 1 TZ2 HLDocument16 pagesMathematics Paper 1 TZ2 HLPavlos StavropoulosPas encore d'évaluation
- Marketing PlanDocument41 pagesMarketing PlanMark AbainzaPas encore d'évaluation
- Enunciado de La Pregunta: Finalizado Se Puntúa 1.00 Sobre 1.00Document9 pagesEnunciado de La Pregunta: Finalizado Se Puntúa 1.00 Sobre 1.00Samuel MojicaPas encore d'évaluation
- Calendar of Cases (May 3, 2018)Document4 pagesCalendar of Cases (May 3, 2018)Roy BacaniPas encore d'évaluation
- Blunders and How To Avoid Them Dunnington PDFDocument147 pagesBlunders and How To Avoid Them Dunnington PDFrajveer404100% (2)
- Thesis FulltextDocument281 pagesThesis FulltextEvgenia MakantasiPas encore d'évaluation
- Public International Law Green Notes 2015Document34 pagesPublic International Law Green Notes 2015KrisLarr100% (1)
- RubricsDocument1 pageRubricsBeaMaeAntoniPas encore d'évaluation
- Reported Speech StatementsDocument1 pageReported Speech StatementsEmilijus Bartasevic100% (1)
- Large Span Structure: MMBC-VDocument20 pagesLarge Span Structure: MMBC-VASHFAQPas encore d'évaluation
- MCN Drill AnswersDocument12 pagesMCN Drill AnswersHerne Balberde100% (1)
- Insomnii, Hipersomnii, ParasomniiDocument26 pagesInsomnii, Hipersomnii, ParasomniiSorina TatuPas encore d'évaluation
- Reith 2020 Lecture 1 TranscriptDocument16 pagesReith 2020 Lecture 1 TranscriptHuy BuiPas encore d'évaluation
- Scatchell Jr. V Village of Melrose Park Et Al.Document48 pagesScatchell Jr. V Village of Melrose Park Et Al.Gianna ScatchellPas encore d'évaluation
- Gandhi Was A British Agent and Brought From SA by British To Sabotage IndiaDocument6 pagesGandhi Was A British Agent and Brought From SA by British To Sabotage Indiakushalmehra100% (2)
- Assignment Class X Arithmetic Progression: AnswersDocument1 pageAssignment Class X Arithmetic Progression: AnswersCRPF SchoolPas encore d'évaluation
- Barangay Sindalan v. CA G.R. No. 150640, March 22, 2007Document17 pagesBarangay Sindalan v. CA G.R. No. 150640, March 22, 2007FD BalitaPas encore d'évaluation
- Peri Operative Nursing ManagementDocument19 pagesPeri Operative Nursing ManagementSabina KontehPas encore d'évaluation
- Finding The NTH Term of An Arithmetic SequenceDocument3 pagesFinding The NTH Term of An Arithmetic SequenceArdy PatawaranPas encore d'évaluation
- ''Want To Learn To Speak Latin or Greek This (2018) Summer''Document10 pages''Want To Learn To Speak Latin or Greek This (2018) Summer''ThriwPas encore d'évaluation
- Essay EnglishDocument4 pagesEssay Englishkiera.kassellPas encore d'évaluation
- Foxit PhantomPDF For HP - Quick GuideDocument32 pagesFoxit PhantomPDF For HP - Quick GuidekhilmiPas encore d'évaluation