Vous aimerez peut-être aussi
- Trainees SIM 2018 ED To PCI ArrestDocument6 pagesTrainees SIM 2018 ED To PCI Arrestmarius vaidaPas encore d'évaluation
- Clinical Handbook of Cardiac ElectrophysiologyD'EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverPas encore d'évaluation
- Acute Respiratory Distress: Section I: Scenario DemographicsDocument6 pagesAcute Respiratory Distress: Section I: Scenario DemographicsharasthaPas encore d'évaluation
- Pediatric DKA: Section I: Scenario DemographicsDocument7 pagesPediatric DKA: Section I: Scenario DemographicsSugi DenyPas encore d'évaluation
- Pediatric DKA: Section I: Scenario DemographicsDocument7 pagesPediatric DKA: Section I: Scenario DemographicsSugi DenyPas encore d'évaluation
- Anaphylaxis With Angioedema: Section I: Scenario DemographicsDocument7 pagesAnaphylaxis With Angioedema: Section I: Scenario DemographicsharasthaPas encore d'évaluation
- Pediatric Septic ShockDocument6 pagesPediatric Septic ShockSugi DenyPas encore d'évaluation
- Trauma: HX and PE (Adults) : For The EMS Providers, (Prior To Patient'sDocument3 pagesTrauma: HX and PE (Adults) : For The EMS Providers, (Prior To Patient'sJustine CastilloPas encore d'évaluation
- Hypovolemic Shock: An OverviewDocument18 pagesHypovolemic Shock: An OverviewVitória PinhoPas encore d'évaluation
- MedED Portal Case ExampleDocument8 pagesMedED Portal Case Examplea6909330Pas encore d'évaluation
- 10em Trauma Case 1Document7 pages10em Trauma Case 1bashayer hamadPas encore d'évaluation
- Medicine: Brachial Plexus Schwannoma Mimicking Cervical LymphadenopathyDocument4 pagesMedicine: Brachial Plexus Schwannoma Mimicking Cervical LymphadenopathykalixinPas encore d'évaluation
- Caso Clinico 3 CompressedDocument20 pagesCaso Clinico 3 Compressedapi-703195004Pas encore d'évaluation
- Farly Ihsan, S.Kep, .Ners Seminar - 28.06.2020 - International - Initial Assesment - Tangerang WEBINAR 28062020Document55 pagesFarly Ihsan, S.Kep, .Ners Seminar - 28.06.2020 - International - Initial Assesment - Tangerang WEBINAR 28062020Endang CandraPas encore d'évaluation
- Emergency Medical Care For Trauma at The Pre-Hospital StageDocument125 pagesEmergency Medical Care For Trauma at The Pre-Hospital StageAkash KumarPas encore d'évaluation
- Simulation Scenario TemplateDocument2 pagesSimulation Scenario Templateapi-258761055100% (1)
- Lecture 2 - ATLS Engl2023Document156 pagesLecture 2 - ATLS Engl2023Swetha K MenonPas encore d'évaluation
- Coventry 06.2012Document14 pagesCoventry 06.2012karan270Pas encore d'évaluation
- EmailingMedPulse 2 5 8Document4 pagesEmailingMedPulse 2 5 8Satyaja KinnaraPas encore d'évaluation
- Code Blue Simulation GuideDocument13 pagesCode Blue Simulation GuideStephanie LiauPas encore d'évaluation
- English Task The Summery of Health Illness, Part of The Body, Medical Practicioners, Oncology and X-Ray & CT ScanDocument7 pagesEnglish Task The Summery of Health Illness, Part of The Body, Medical Practicioners, Oncology and X-Ray & CT ScanYudha HupayantiPas encore d'évaluation
- MRCS StationsDocument6 pagesMRCS StationsAnirban Ghosh0% (1)
- Self-Extrication and Selective Spinal Immobilisation in A Polytrauma Patient With Spinal InjuriesDocument4 pagesSelf-Extrication and Selective Spinal Immobilisation in A Polytrauma Patient With Spinal InjuriesLeandro NogueiraPas encore d'évaluation
- Case Study 55Document35 pagesCase Study 55xWinTedPas encore d'évaluation
- This Study Resource Was: Assessment & Reasoning Cardiac SystemDocument6 pagesThis Study Resource Was: Assessment & Reasoning Cardiac SystemSharon TanveerPas encore d'évaluation
- Nursing Iv The Secondary Survey in Basic Cardiac Life Support (BCLS)Document14 pagesNursing Iv The Secondary Survey in Basic Cardiac Life Support (BCLS)Ni wayan mirayantiPas encore d'évaluation
- Secondary SurveyDocument14 pagesSecondary SurveyNi wayan mirayantiPas encore d'évaluation
- Lesson Plan Lumbar PunctureDocument25 pagesLesson Plan Lumbar PunctureValarmathi50% (4)
- Percussion Pacing - An Almost Forgotten Procedure For Haemodynamically Unstable Bradycardias A Report of Three Case Studies and Review of The LiteratureDocument5 pagesPercussion Pacing - An Almost Forgotten Procedure For Haemodynamically Unstable Bradycardias A Report of Three Case Studies and Review of The LiteratureLiliannePas encore d'évaluation
- Ortho HO Exam NS AnswerDocument33 pagesOrtho HO Exam NS Answersarvesswara muniandyPas encore d'évaluation
- Triada de CharcotDocument1 pageTriada de Charcotdanitza pilcoPas encore d'évaluation
- Placing A Lumbar Epidural CatheterDocument4 pagesPlacing A Lumbar Epidural CatheterGus LionsPas encore d'évaluation
- Iatrogenic Horner Syndrome: Etiology, Diagnosis and OutcomesDocument2 pagesIatrogenic Horner Syndrome: Etiology, Diagnosis and OutcomesEldi Saut Maduma NainggolanPas encore d'évaluation
- CR - RamirezDocument4 pagesCR - RamirezTommysPas encore d'évaluation
- ATLS Case ScenarioDocument13 pagesATLS Case ScenarioJenny Schneider100% (2)
- ATLS (Advanced Trauma Life Support) Teaching Protocol Pretest (30 Min) Context of Tutorial (2 Hours)Document22 pagesATLS (Advanced Trauma Life Support) Teaching Protocol Pretest (30 Min) Context of Tutorial (2 Hours)Zitaputri BundaPas encore d'évaluation
- Medical Devices of The ChestDocument22 pagesMedical Devices of The ChestJose David Flores PérezPas encore d'évaluation
- Shock HypovolemicDocument19 pagesShock HypovolemicChance Jackson100% (1)
- Idiopathic Cervical Spinal Subdural Haematoma: A Case Report and Literature ReviewDocument10 pagesIdiopathic Cervical Spinal Subdural Haematoma: A Case Report and Literature ReviewSelfa YunitaPas encore d'évaluation
- Multiple Trauma TKVDocument21 pagesMultiple Trauma TKVKahfi RakhmadianPas encore d'évaluation
- ATLS (Advanced Trauma Life Support) Teaching Protocol Pretest (30 Min) Context of Tutorial (2 Hours)Document16 pagesATLS (Advanced Trauma Life Support) Teaching Protocol Pretest (30 Min) Context of Tutorial (2 Hours)anon_778118144Pas encore d'évaluation
- A Giant Spinal Arterial Aneurysm in A Child Presenting As Quadriparesis (Case Reports, Vol. 2013, Issue Aug20 1) (2013)Document4 pagesA Giant Spinal Arterial Aneurysm in A Child Presenting As Quadriparesis (Case Reports, Vol. 2013, Issue Aug20 1) (2013)negin.safari8227Pas encore d'évaluation
- TPSVDocument28 pagesTPSVGeraldine CortesPas encore d'évaluation
- J Jhsa 2017 10 014Document5 pagesJ Jhsa 2017 10 014Nicolas AdrianoPas encore d'évaluation
- JobsRegistrationDownloads File 1Document8 pagesJobsRegistrationDownloads File 1Amanda LaPointPas encore d'évaluation
- December 2008final FRCA VivaDocument43 pagesDecember 2008final FRCA Vivajahangirealam100% (2)
- Emergent Conditions (Triage and CPR)Document4 pagesEmergent Conditions (Triage and CPR)mikErlhPas encore d'évaluation
- Integrasi Igd Aortic DissectionDocument21 pagesIntegrasi Igd Aortic Dissectionrahageng wida kusumaPas encore d'évaluation
- Final Submited Meningomyelocele101010Document13 pagesFinal Submited Meningomyelocele101010agumasPas encore d'évaluation
- Jerash University Faculty of Nursing Critical Care Nursing Practicum Case StudyDocument9 pagesJerash University Faculty of Nursing Critical Care Nursing Practicum Case StudytasneemPas encore d'évaluation
- Stroke Hemorrhagic ScenarioDocument16 pagesStroke Hemorrhagic ScenarioAri ErfandiPas encore d'évaluation
- Carpal Tunnel Syndrome: An Update For The Primary Care PhysicianDocument5 pagesCarpal Tunnel Syndrome: An Update For The Primary Care PhysicianNovia KurniantiPas encore d'évaluation
- Radiology Class:: Brain and ChestDocument76 pagesRadiology Class:: Brain and ChestNurul NajwaPas encore d'évaluation
- External HydrocephalusDocument8 pagesExternal HydrocephalusJorge VergaraPas encore d'évaluation
- Pathological FractureDocument92 pagesPathological FractureSeptyAuliaPas encore d'évaluation
- Vertebral Artery DissectionDocument40 pagesVertebral Artery DissectionJeevankumar DommarajuPas encore d'évaluation
- Dacheng Jin 2020Document5 pagesDacheng Jin 2020Nehemias MD GuevaraPas encore d'évaluation
- B20M3L5 - Neck InjuriesDocument4 pagesB20M3L5 - Neck InjuriesBarda GulanPas encore d'évaluation
- Group Courage - Multiple Injured Patient (Case Discussion)Document19 pagesGroup Courage - Multiple Injured Patient (Case Discussion)Jimmy V. Venturina, Jr.Pas encore d'évaluation
- Medicina 57 00312 v3Document16 pagesMedicina 57 00312 v3harasthaPas encore d'évaluation
- Regional Anaesthesia To Prevent Chronic Pain After Surgery: A Cochrane Systematic Review and Meta-AnalysisDocument10 pagesRegional Anaesthesia To Prevent Chronic Pain After Surgery: A Cochrane Systematic Review and Meta-AnalysisharasthaPas encore d'évaluation
- Postmastectomy and Postthoracotomy Pain: Anne M. Wallace, MD, and Mark S. Wallace, MDDocument18 pagesPostmastectomy and Postthoracotomy Pain: Anne M. Wallace, MD, and Mark S. Wallace, MDharasthaPas encore d'évaluation
- Opioid-Induced Tolerance and HyperalgesiaDocument70 pagesOpioid-Induced Tolerance and HyperalgesiaharasthaPas encore d'évaluation
- Jurnal Anastesi - The Role of Continous Peripheral Nerve BlocksDocument20 pagesJurnal Anastesi - The Role of Continous Peripheral Nerve BlocksMichele JohnsonPas encore d'évaluation
- JPR 8 009Document13 pagesJPR 8 009harasthaPas encore d'évaluation
- No.6 Tzellos2008Document8 pagesNo.6 Tzellos2008harasthaPas encore d'évaluation
- Paravetebral EpiduralDocument7 pagesParavetebral EpiduralharasthaPas encore d'évaluation
- Dialysis in Critically IllDocument48 pagesDialysis in Critically IllFate ChanPas encore d'évaluation
- LectureDocument4 pagesLectureharasthaPas encore d'évaluation
- HOW TO Assess For Pain Sensitisation in The Clinic HANDOUTDocument12 pagesHOW TO Assess For Pain Sensitisation in The Clinic HANDOUTharasthaPas encore d'évaluation
- 03.laboratory Testing Related COVID-19 MF04042020Document61 pages03.laboratory Testing Related COVID-19 MF04042020mulyadi diningrum100% (1)
- Peripheral Chemical Mediators of Pain and HyperalgesiaDocument1 pagePeripheral Chemical Mediators of Pain and HyperalgesiaharasthaPas encore d'évaluation
- Acog AccretaDocument17 pagesAcog AccretaharasthaPas encore d'évaluation
- 1 PBDocument6 pages1 PBAustine OsawePas encore d'évaluation
- 9d18 PDFDocument22 pages9d18 PDFharasthaPas encore d'évaluation
- International Journal of Anesthetics and Anesthesiology Ijaa 3 052Document9 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 3 052harasthaPas encore d'évaluation
- Craniocervical Dystonia Blepharospasm. Spasmodic Contraction of TheDocument3 pagesCraniocervical Dystonia Blepharospasm. Spasmodic Contraction of TheharasthaPas encore d'évaluation
- Caesarean Section1846Document12 pagesCaesarean Section1846harasthaPas encore d'évaluation
- Endothelial Glycocalyx: Role in Body Fluid Homeostasis and Fluid ManagementDocument9 pagesEndothelial Glycocalyx: Role in Body Fluid Homeostasis and Fluid ManagementharasthaPas encore d'évaluation
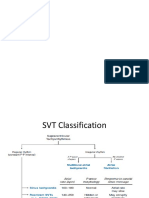
- SVTDocument21 pagesSVTharasthaPas encore d'évaluation
- 4.5 THE TREATMENT OF CONGENITAL HYDROCEPHALUS. M.J. Joubert PDFDocument3 pages4.5 THE TREATMENT OF CONGENITAL HYDROCEPHALUS. M.J. Joubert PDFharasthaPas encore d'évaluation
- Managing Advanced PD PDFDocument29 pagesManaging Advanced PD PDFharasthaPas encore d'évaluation
- Pengaruh Anestesi Regional Dan General Pada Sectio Cesaria Pada Ibu Dengan Pre Eklampsia Berat Terhadap Apgar ScoreDocument12 pagesPengaruh Anestesi Regional Dan General Pada Sectio Cesaria Pada Ibu Dengan Pre Eklampsia Berat Terhadap Apgar ScoreMuhamad Ongky NRahardiPas encore d'évaluation
- MorphineDocument16 pagesMorphineharasthaPas encore d'évaluation
- MorphineDocument16 pagesMorphineharasthaPas encore d'évaluation
- Brusselle - Immunology of COPD - Review - Lancet 2011 PDFDocument12 pagesBrusselle - Immunology of COPD - Review - Lancet 2011 PDFharasthaPas encore d'évaluation
- Mortality Predictors in SepsisDocument5 pagesMortality Predictors in SepsisharasthaPas encore d'évaluation
- Mortality Predictors in SepsisDocument5 pagesMortality Predictors in SepsisharasthaPas encore d'évaluation
- Breech NRPDocument8 pagesBreech NRPharasthaPas encore d'évaluation
- Question BankDocument6 pagesQuestion Bankkoang lual gachPas encore d'évaluation
- Terapi CompressionDocument10 pagesTerapi CompressionErlinda KarimPas encore d'évaluation
- Heart (CVS) : Pericardium / Pericardial SacDocument7 pagesHeart (CVS) : Pericardium / Pericardial SacMarjorie ViescaPas encore d'évaluation
- Dynamic AuscultationDocument47 pagesDynamic AuscultationSrinivas PingaliPas encore d'évaluation
- Physiological Origin of Biomedical SignalDocument35 pagesPhysiological Origin of Biomedical Signalsouvik5000100% (1)
- Unit 3 Problem 2Document8 pagesUnit 3 Problem 2Adoub AlderaziPas encore d'évaluation
- Priority Problem For Severe Hypertension: Nursing Care PlanDocument3 pagesPriority Problem For Severe Hypertension: Nursing Care PlanDeanne MunarPas encore d'évaluation
- Dead On ArrivalDocument35 pagesDead On ArrivalFitria Diah Suharjo100% (1)
- CVK Kod Djece, DužinaDocument4 pagesCVK Kod Djece, DužinaDamir PištoljevićPas encore d'évaluation
- 0 - Anesthetic Management of A Case With Aortic Regurgitation Posted For Laproscopic Hernia Mesh RepairDocument4 pages0 - Anesthetic Management of A Case With Aortic Regurgitation Posted For Laproscopic Hernia Mesh RepairAromal SatheeshPas encore d'évaluation
- Evaluating Stable Chest Pain - An Evolving Approach: EditorialDocument2 pagesEvaluating Stable Chest Pain - An Evolving Approach: EditorialMahmoud AbouelsoudPas encore d'évaluation
- 100 ECG For AKP - With AnswersDocument102 pages100 ECG For AKP - With AnswersaeyousefPas encore d'évaluation
- ACLS Answer KeyDocument23 pagesACLS Answer KeyKirana Budhiarta94% (17)
- FORENSIC 5 WEEK 4 Students Copy 2023Document68 pagesFORENSIC 5 WEEK 4 Students Copy 2023Grczhl GornesPas encore d'évaluation
- Pijat Kaki THD HipertensiDocument8 pagesPijat Kaki THD Hipertensidedi wahyudinPas encore d'évaluation
- National Model EMS Clinical Guidelines Version2 Sept2017Document373 pagesNational Model EMS Clinical Guidelines Version2 Sept2017epraetorianPas encore d'évaluation
- Pacemaker 180508042454Document86 pagesPacemaker 180508042454padmaPas encore d'évaluation
- Repet cz1 U8 Tests Answer Key and AudioscriptDocument3 pagesRepet cz1 U8 Tests Answer Key and Audioscriptmiloszez108Pas encore d'évaluation
- Fasting Insulin Levels Independently Associates With Coronary Heart Diseade in Non-Diabetic Turkish Men and WomenDocument9 pagesFasting Insulin Levels Independently Associates With Coronary Heart Diseade in Non-Diabetic Turkish Men and WomenJanne AraújoPas encore d'évaluation
- Tanggal Rujuk BalnamaDocument7 pagesTanggal Rujuk BalnamapkmjemursariPas encore d'évaluation
- Antiadrenergic Drugs - II 24.07.018 PDFDocument25 pagesAntiadrenergic Drugs - II 24.07.018 PDFHitesh karnPas encore d'évaluation
- Angina Pectoris & Anti Anginal DrugsDocument46 pagesAngina Pectoris & Anti Anginal DrugsMohammad AliPas encore d'évaluation
- Management of Hypertensive Elderly in Clinical Dentistry: Patcharaphol Samnieng, Kantapong PloydanaiDocument9 pagesManagement of Hypertensive Elderly in Clinical Dentistry: Patcharaphol Samnieng, Kantapong PloydanaiSatya AsatyaPas encore d'évaluation
- Lesson 1 - Module 1 - Circulatory SystemDocument27 pagesLesson 1 - Module 1 - Circulatory SystemPapiPas encore d'évaluation
- What Is Atrial FibrillationDocument3 pagesWhat Is Atrial FibrillationMoni ShafiqPas encore d'évaluation
- Surviving Sepsis GuidelinesDocument17 pagesSurviving Sepsis GuidelinesNabil RohaizatPas encore d'évaluation
- IMANE 2020 presentation - Reconstruction of aTAA - (ΕΛΚΕ)Document12 pagesIMANE 2020 presentation - Reconstruction of aTAA - (ΕΛΚΕ)Nikos VaxevanidisPas encore d'évaluation
- Norepinephrine FinalDocument2 pagesNorepinephrine FinalNelly CruzPas encore d'évaluation
- Discharge Audit For AMAU: Instructions For Audit ToolDocument37 pagesDischarge Audit For AMAU: Instructions For Audit Toolpioneer92Pas encore d'évaluation
- Percutaneous Transluminal Coronary AngioplastyDocument22 pagesPercutaneous Transluminal Coronary AngioplastyArya Gaunker100% (1)