Vous aimerez peut-être aussi
- Blue Veins Sub Theme TVBDocument4 pagesBlue Veins Sub Theme TVB1234chocoPas encore d'évaluation
- Doctor Talk: Communication Practice Role PlaysDocument6 pagesDoctor Talk: Communication Practice Role Plays1234chocoPas encore d'évaluation
- Code Geass - StoriesDocument5 pagesCode Geass - Stories1234chocoPas encore d'évaluation
- Pokemon Theme Song 22Document4 pagesPokemon Theme Song 221234chocoPas encore d'évaluation
- Mbs Quick Guide: JULY 2020Document2 pagesMbs Quick Guide: JULY 20201234chocoPas encore d'évaluation
- Osteo Infographic FinalDocument1 pageOsteo Infographic Final1234chocoPas encore d'évaluation
- Fairy Tail - Main ThemeDocument3 pagesFairy Tail - Main Theme1234chocoPas encore d'évaluation
- Topical Steroids (Sep 19) PDFDocument7 pagesTopical Steroids (Sep 19) PDF1234chocoPas encore d'évaluation
- QLD Rail Traim PDFDocument1 pageQLD Rail Traim PDF1234chocoPas encore d'évaluation
- # 3 - Prospective Study of The Diagnostic Accuracy of The Simplify D-Dimer Assay For Pulmonary Embolism in EDDocument7 pages# 3 - Prospective Study of The Diagnostic Accuracy of The Simplify D-Dimer Assay For Pulmonary Embolism in ED1234chocoPas encore d'évaluation
- Blue BirdDocument7 pagesBlue Bird1234chocoPas encore d'évaluation
- Topical Steroids (Sep 19) PDFDocument7 pagesTopical Steroids (Sep 19) PDF1234chocoPas encore d'évaluation
- PBM Module1 MTP Template 0Document2 pagesPBM Module1 MTP Template 01234chocoPas encore d'évaluation
- Getting the Hospital Job: A Step-by-Step Guide to Applying for Your First PositionDocument41 pagesGetting the Hospital Job: A Step-by-Step Guide to Applying for Your First Position1234chocoPas encore d'évaluation
- USMLE Flashcards: Anatomy - Side by SideDocument190 pagesUSMLE Flashcards: Anatomy - Side by SideMedSchoolStuff100% (3)
- FLOWCHART - ARC Adult Cardiorespiratory ArrestDocument1 pageFLOWCHART - ARC Adult Cardiorespiratory Arrest1234chocoPas encore d'évaluation
- Acute Low Back Pain Flowchart January 2017Document1 pageAcute Low Back Pain Flowchart January 20171234chocoPas encore d'évaluation
- 2016 Applicant Guide Web V2Document83 pages2016 Applicant Guide Web V21234chocoPas encore d'évaluation
- Fluids ElectrolytesDocument2 pagesFluids Electrolytes1234chocoPas encore d'évaluation
- Metro South Intern Training Form (Logan)Document3 pagesMetro South Intern Training Form (Logan)1234chocoPas encore d'évaluation
- Taking a Social and Cultural History: A Biopsychosocial ApproachDocument3 pagesTaking a Social and Cultural History: A Biopsychosocial Approach1234chocoPas encore d'évaluation
- Managing Mental Illness in Patients From CALD Backgrounds: PsychiatryDocument5 pagesManaging Mental Illness in Patients From CALD Backgrounds: Psychiatry1234chocoPas encore d'évaluation
- The Effects of Social Networks On Disability in Older AustraliansDocument22 pagesThe Effects of Social Networks On Disability in Older Australians1234chocoPas encore d'évaluation
- Herd Immunity'' A Rough Guide PDFDocument6 pagesHerd Immunity'' A Rough Guide PDF1234chocoPas encore d'évaluation
- Language of PreventionDocument9 pagesLanguage of Prevention1234chocoPas encore d'évaluation
- Defining and Assessing Risks To Health PDFDocument20 pagesDefining and Assessing Risks To Health PDF1234chocoPas encore d'évaluation
- Clinical Contributions To Addressing The Social Determinants of HealthDocument5 pagesClinical Contributions To Addressing The Social Determinants of Health1234chocoPas encore d'évaluation
- ImprovingMedAdherenceOlderAdultslyer Final 508CDocument2 pagesImprovingMedAdherenceOlderAdultslyer Final 508CKumar PatilPas encore d'évaluation
- A Conceptual Framework For HealthDocument1 pageA Conceptual Framework For Health1234chocoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Dangerous drug prescription errorsDocument2 pagesDangerous drug prescription errorsCASSEY ANNE LARAPas encore d'évaluation
- 2016 Guidelines For The Management of Thyroid StorDocument41 pages2016 Guidelines For The Management of Thyroid StorStella Gracia OctaricaPas encore d'évaluation
- Aromatherapy The Practice of Aromas in UDocument7 pagesAromatherapy The Practice of Aromas in UAbdul Jalil HridoyPas encore d'évaluation
- Principles of Antibiotic Formulary Selection For P&T Committees 1Document3 pagesPrinciples of Antibiotic Formulary Selection For P&T Committees 1madengPas encore d'évaluation
- Lactone Glycosides and Lipids SummaryDocument3 pagesLactone Glycosides and Lipids SummaryAntonio CharismaPas encore d'évaluation
- Foxglove: Student Name: Strugariu Eisenhauer Eduard AlexDocument9 pagesFoxglove: Student Name: Strugariu Eisenhauer Eduard AlexStrugariu Eisenhauer Eduard AlexPas encore d'évaluation
- Academic Emergency Medicine - 2017 - Zahed - Topical Tranexamic Acid Compared With Anterior Nasal Packing For Treatment ofDocument8 pagesAcademic Emergency Medicine - 2017 - Zahed - Topical Tranexamic Acid Compared With Anterior Nasal Packing For Treatment ofathallaPas encore d'évaluation
- Merck & Co., Inc. (A) ConvertttDocument5 pagesMerck & Co., Inc. (A) ConvertttvdrtPas encore d'évaluation
- Welcome To The Transpharma® Sale!: Canada's Leader in Performance ProductsDocument3 pagesWelcome To The Transpharma® Sale!: Canada's Leader in Performance ProductsderrickPas encore d'évaluation
- Calcium Gluconate Adult IV MonographDocument2 pagesCalcium Gluconate Adult IV MonographRafiq Esufzae0% (1)
- IMRD Workng Paper TemplateDocument28 pagesIMRD Workng Paper TemplateFrancezkaPaulaPapaPas encore d'évaluation
- IbandronateDocument2 pagesIbandronatePratik R JobaliaPas encore d'évaluation
- Data Ba RangDocument180 pagesData Ba Rangsherly damayantiPas encore d'évaluation
- Terapi FluDocument15 pagesTerapi FluRama DayantiPas encore d'évaluation
- Rice Black Bug Control Using Tubli Root ExtractDocument26 pagesRice Black Bug Control Using Tubli Root ExtractJan Angela BaylonPas encore d'évaluation
- Gastroenterology by Elagouri MohammedDocument31 pagesGastroenterology by Elagouri MohammedStylesh GuRlyPas encore d'évaluation
- In Vitro Anti Arthritic Activity of Acacia Catechu WilldDocument3 pagesIn Vitro Anti Arthritic Activity of Acacia Catechu WilldEditor IJTSRDPas encore d'évaluation
- The Therapeutic Potential of Apelin in Kidney DiseaseDocument14 pagesThe Therapeutic Potential of Apelin in Kidney DiseasecastillojessPas encore d'évaluation
- Stab Wound PathophysiologyDocument5 pagesStab Wound PathophysiologyJaessa Feliciano86% (7)
- 1 s2.0 S0014488621001849 MainDocument14 pages1 s2.0 S0014488621001849 MainGregory AssonitisPas encore d'évaluation
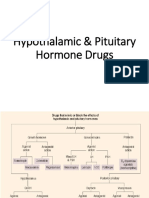
- Hypothalamic & Pituitary Hormone DrugsDocument29 pagesHypothalamic & Pituitary Hormone DrugsDylan MansillaPas encore d'évaluation
- Bloody Easy - Coagulation ExplainedDocument25 pagesBloody Easy - Coagulation ExplainedDaniela GreerePas encore d'évaluation
- Supriya Lifescience Limited Regulatory 1441025790Document2 pagesSupriya Lifescience Limited Regulatory 1441025790Yergali AmanzholPas encore d'évaluation
- Suvarna 2015Document7 pagesSuvarna 2015Lívia MeloPas encore d'évaluation
- Bisoprolol and Kidney FunctionDocument11 pagesBisoprolol and Kidney FunctionZahid MahmoodPas encore d'évaluation
- 100 Dosage Calculation Practice Problems AnswersDocument12 pages100 Dosage Calculation Practice Problems AnswersTeena Real81% (21)
- NO Jenis Penya KIT Nama ObatDocument7 pagesNO Jenis Penya KIT Nama ObatVina PrihartatiPas encore d'évaluation
- Pharmacology in EndodonticsDocument9 pagesPharmacology in EndodonticsIJAR JOURNALPas encore d'évaluation
- Use of Antibiotic and Analgesic Drugs During LactationDocument11 pagesUse of Antibiotic and Analgesic Drugs During LactationpinakshiPas encore d'évaluation
- Amantadine Uses, Dosage, Side Effects, WarningsDocument6 pagesAmantadine Uses, Dosage, Side Effects, WarningspatgarettPas encore d'évaluation